

A computerized provider order entry intervention for medication safety during acute kidney injury: a quality improvement report
- PMID: 20709437
- PMCID: PMC2963668
- DOI: 10.1053/j.ajkd.2010.05.024
A computerized provider order entry intervention for medication safety during acute kidney injury: a quality improvement report
Abstract
Background: Frequently, prescribers fail to account for changing kidney function when prescribing medications. We evaluated the use of a computerized provider order entry intervention to improve medication management during acute kidney injury.
Study design: Quality improvement report with time series analyses.
Setting & participants: 1,598 adult inpatients with a minimum 0.5-mg/dL increase in serum creatinine level over 48 hours after an order for at least one of 122 nephrotoxic or renally cleared medications.
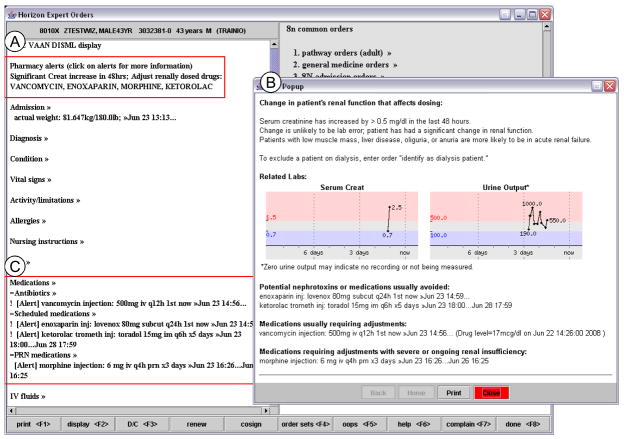
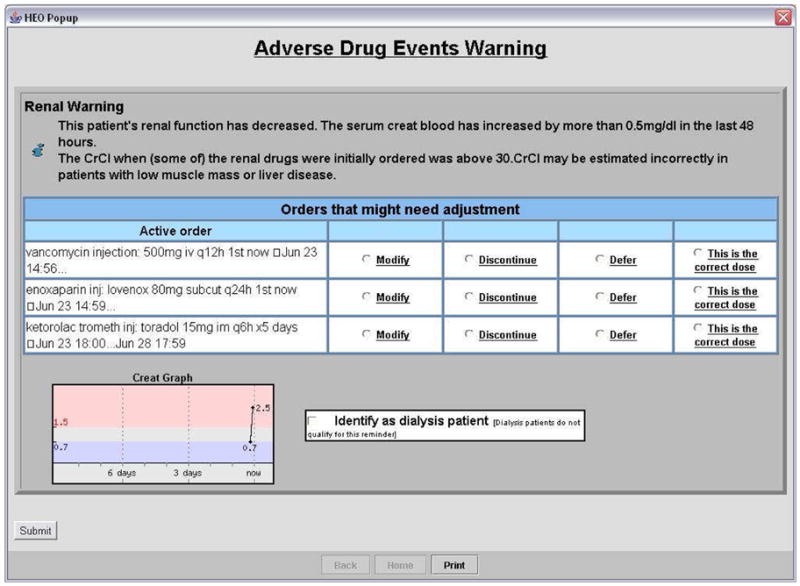
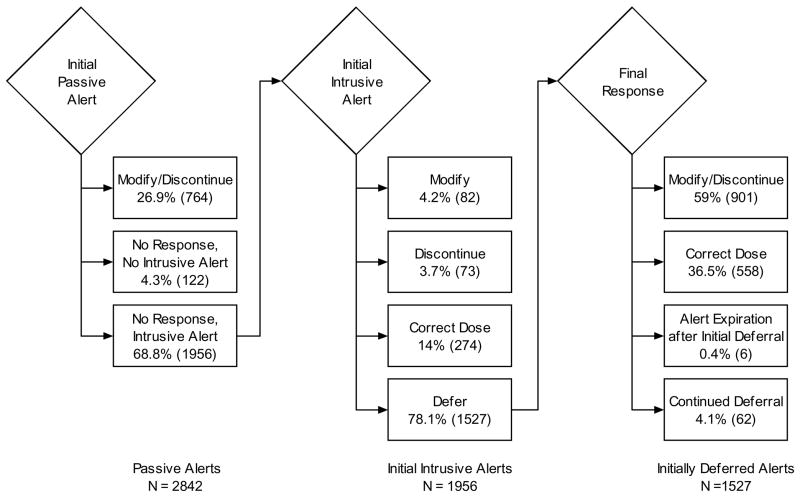
Quality improvement plan: Passive noninteractive warnings about increasing serum creatinine level appeared within the computerized provider order entry interface and on printed rounding reports. For contraindicated or high-toxicity medications that should be avoided or adjusted, an interruptive alert within the system asked providers to modify or discontinue the targeted orders, mark the current dosing as correct and to remain unchanged, or defer the alert to reappear in the next session.
Outcomes & measurements: Intervention effect on drug modification or discontinuation, time to modification or discontinuation, and provider interactions with alerts.
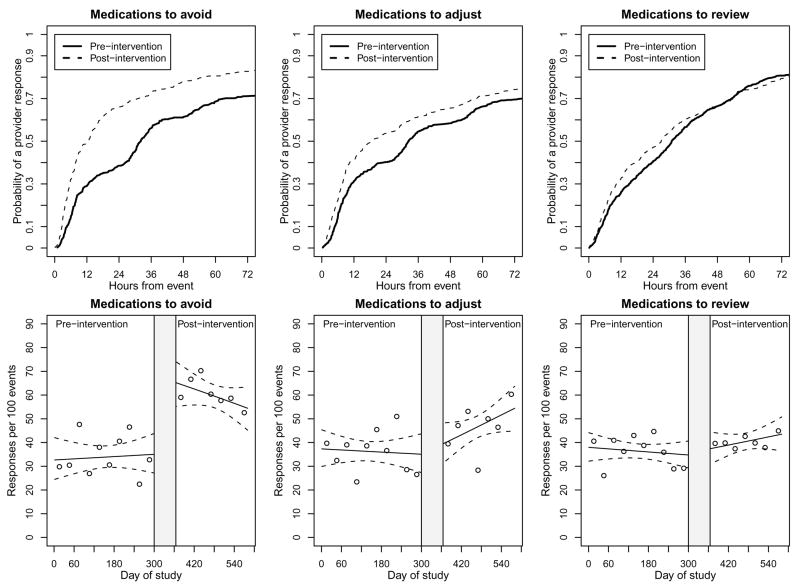
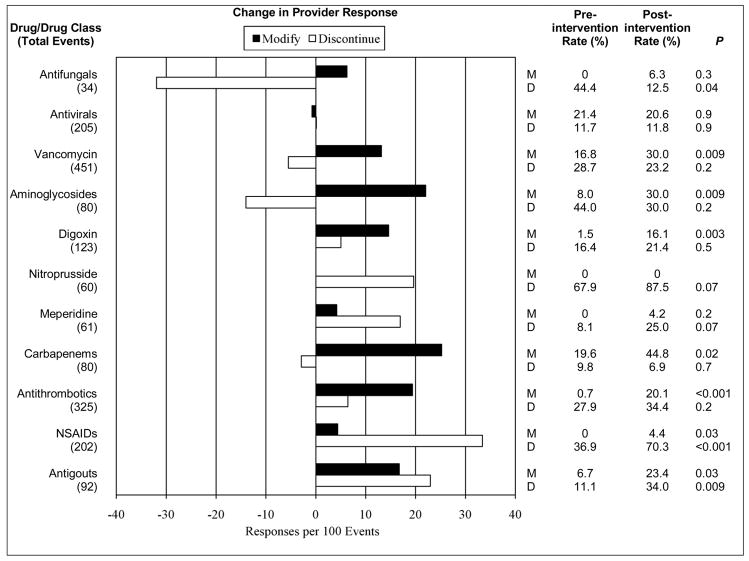
Results: The modification or discontinuation rate per 100 events for medications included in the interruptive alert within 24 hours of increasing creatinine level improved from 35.2 preintervention to 52.6 postintervention (P < 0.001); orders were modified or discontinued more quickly (P < 0.001). During the postintervention period, providers initially deferred 78.1% of interruptive alerts, although 54% of these eventually were modified or discontinued before patient death, discharge, or transfer. The response to passive alerts about medications requiring review did not significantly change compared with baseline.
Limitations: Single tertiary-care academic medical center; provider actions were not independently adjudicated for appropriateness.
Conclusions: A computerized provider order entry-based alerting system to support medication management after acute kidney injury significantly increased the rate and timeliness of modification or discontinuation of targeted medications.
Copyright © 2010 National Kidney Foundation, Inc. All rights reserved.
Figures
Comment in
-
Using computerized provider order entry and clinical decision support to improve prescribing in patients with decreased GFR.Am J Kidney Dis. 2010 Nov;56(5):809-12. doi: 10.1053/j.ajkd.2010.09.006. Am J Kidney Dis. 2010. PMID: 20970021 No abstract available.
References
-
- Clermont G, Acker CG, Angus DC, et al. Renal failure in the ICU: comparison of the impact of acute renal failure and end-stage renal disease on ICU outcomes. Kidney Int. 2002;62(3):986–996. - PubMed
-
- Hou SH, Bushinsky DA, Wish JB, Cohen JJ, Harrington JT. Hospital-acquired renal insufficiency: a prospective study. Am J Med. 1983;74(2):243–248. - PubMed
-
- Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002;39(5):930–936. - PubMed
-
- Cantú TG, Ellerbeck EF, Yun SW, Castine SD, Kornhauser DM. Drug prescribing for patients with changing renal function. Am J Hosp Pharm. 1992;49(12):2944–2948. - PubMed
-
- Menashe PI, Ross SA, Gottlieb JE. Acquired renal insufficiency in critically ill patients. Crit Care Med. 1988;16(11):1106–1109. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
