

Cystatin C, albuminuria, and 5-year all-cause mortality in HIV-infected persons
- PMID: 20709438
- PMCID: PMC3164880
- DOI: 10.1053/j.ajkd.2010.05.019
Cystatin C, albuminuria, and 5-year all-cause mortality in HIV-infected persons
Abstract
Background: Compared with controls, human immunodeficiency virus (HIV)-infected persons have a greater prevalence of kidney disease, assessed according to high cystatin C level and albuminuria, but not according to creatinine level. However, the clinical importance of increased cystatin C level and albuminuria in the HIV-infected population has not been studied.
Study design: We conducted an observational cohort study to determine the association of kidney disease (measured according to albuminuria, cystatin C, and serum creatinine) with mortality.
Setting & participants: 922 HIV-infected persons enrolled in the FRAM (Fat Redistribution and Metabolic Change in HIV Infection) Study.
Predictor: Serum cystatin C and serum creatinine levels were used to estimate glomerular filtration rates (eGFR(SCysC) and eGFR(SCr), respectively). Albuminuria was defined as a positive urine dipstick result (≥ 1+) or urine albumin-creatinine ratio >30 mg/g.
Outcome: 5-Year mortality.
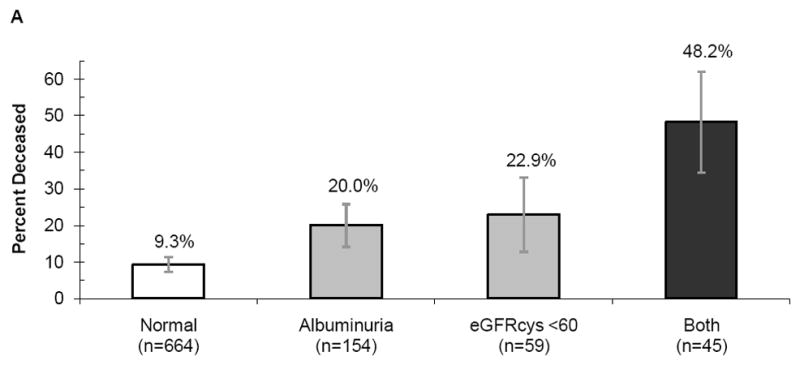
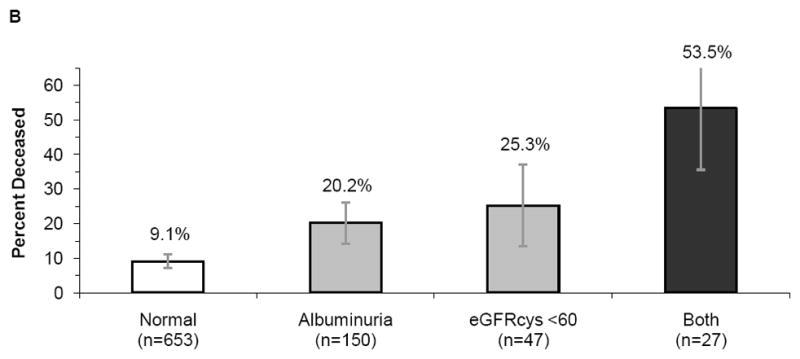
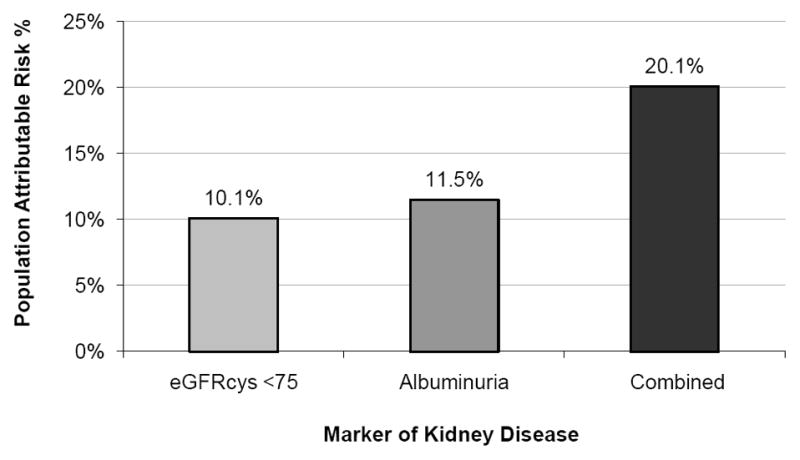
Results: At baseline, decreased kidney function (eGFR(SCysC) <60 mL/min/1.73 m(2)) or albuminuria was present in 28% of participants. After 5 years of follow-up, mortality was 48% in those with both eGFR(SCysC) < 60 mL/min/1.73 m(2) and albuminuria, 23% in those with eGFR(SCysC) < 60 mL/min/1.73 m(2) alone, 20% in those with albuminuria alone, and 9% in those with neither condition. After multivariable adjustment for demographics, cardiovascular risk factors, HIV-related factors, and inflammatory marker levels, eGFR(SCysC) < 60 mL/min/1.73 m(2) and albuminuria were associated with a nearly 2-fold increase in mortality, whereas eGFR(SCr) < 60 mL/min/1.73 m(2) did not appear to have a substantial association with mortality. Together, eGFR(SCysC) <60 mL/min/1.73 m(2) and albuminuria accounted for 17% of the population-level attributable risk of mortality.
Limitations: Vital status was unknown in 261 participants from the original cohort.
Conclusions: Kidney disease marked by albuminuria or increased cystatin C level appears to be an important risk factor for mortality in HIV-infected individuals. A substantial proportion of this risk may be unrecognized because of the current reliance on serum creatinine to estimate kidney function in clinical practice.
Published by Elsevier Inc.
Figures
References
-
- Lohse N, Hansen AB, Pedersen G, et al. Survival of persons with and without HIV infection in Denmark, 1995–2005. Ann Intern Med. 2007 Jan 16;146(2):87–95. - PubMed
-
- Eggers PW, Kimmel PL. Is there an epidemic of HIV Infection in the US ESRD program? J Am Soc Nephrol. 2004 Sep;15(9):2477–2485. - PubMed
-
- Perkins BA, Ficociello LH, Ostrander BE, et al. Microalbuminuria and the Risk for Early Progressive Renal Function Decline in Type 1 Diabetes. J Am Soc Nephrol. 2007 Feb 28; - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P30 AI027767/AI/NIAID NIH HHS/United States
- M01 RR00054/RR/NCRR NIH HHS/United States
- R01 HL53359/HL/NHLBI NIH HHS/United States
- R01 DK057508/DK/NIDDK NIH HHS/United States
- UL1 KL2 RR024130/RR/NCRR NIH HHS/United States
- K23 AI066943/AI/NIAID NIH HHS/United States
- M01 RR000054/RR/NCRR NIH HHS/United States
- M01 RR00865/RR/NCRR NIH HHS/United States
- R01 HL074814/HL/NHLBI NIH HHS/United States
- M01 RR0636/RR/NCRR NIH HHS/United States
- K23 DK080645/DK/NIDDK NIH HHS/United States
- K23 DK080645-01A1/DK/NIDDK NIH HHS/United States
- R01 DK57508/DK/NIDDK NIH HHS/United States
- M01 RR00051/RR/NCRR NIH HHS/United States
- M01 RR000865/RR/NCRR NIH HHS/United States
- M01 RR000036/RR/NCRR NIH HHS/United States
- KL2 RR024130/RR/NCRR NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- K23 AI66943/AI/NIAID NIH HHS/United States
- M01 RR00083/RR/NCRR NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- M01 RR000051/RR/NCRR NIH HHS/United States
- M01 RR00036/RR/NCRR NIH HHS/United States
- M01 RR000083/RR/NCRR NIH HHS/United States
- R01 HL74814/HL/NHLBI NIH HHS/United States
- M01 RR00052/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
