

Who benefits most from mild therapeutic hypothermia in coronary intervention era? A retrospective and propensity-matched study
- PMID: 20712862
- PMCID: PMC2945139
- DOI: 10.1186/cc9225
Who benefits most from mild therapeutic hypothermia in coronary intervention era? A retrospective and propensity-matched study
Abstract
Introduction: The aim of the present study was to investigate the impact of the time interval from collapse to return of spontaneous circulation (CPA-ROSC) in cardiac arrest patients and the types of patients who will benefit from therapeutic hypothermia.
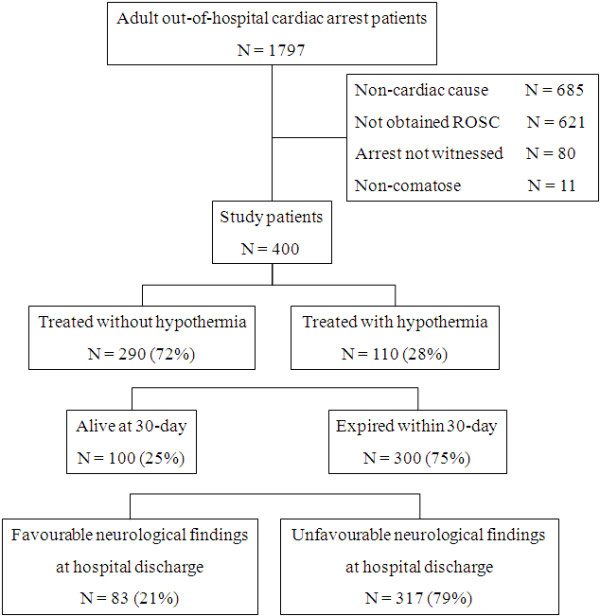
Methods: Four hundred witnessed adult comatose survivors of out-of-hospital cardiac arrest of cardiac etiology were enrolled in the study. The favorable neurological outcome was defined as category 1 or 2 on the five-point Pittsburgh cerebral performance scale at the time of hospital discharge. A matching process based on the propensity score was performed to equalize potential prognostic factors in the hypothermia and normothermia groups, and to formulate a balanced 1:1 matched cohort study.
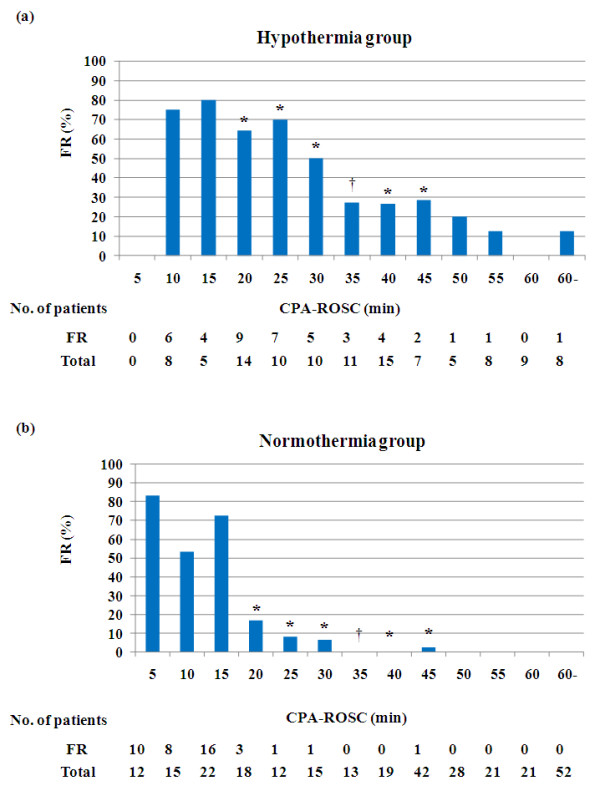
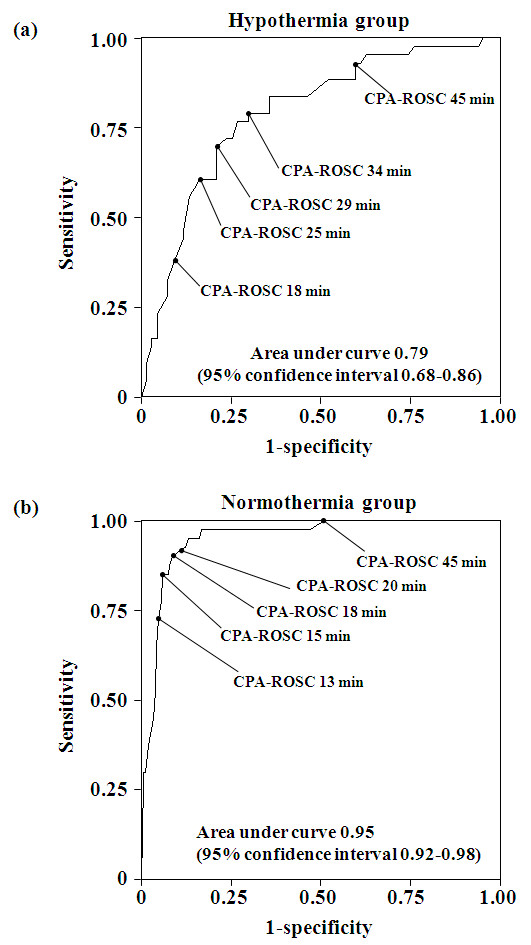
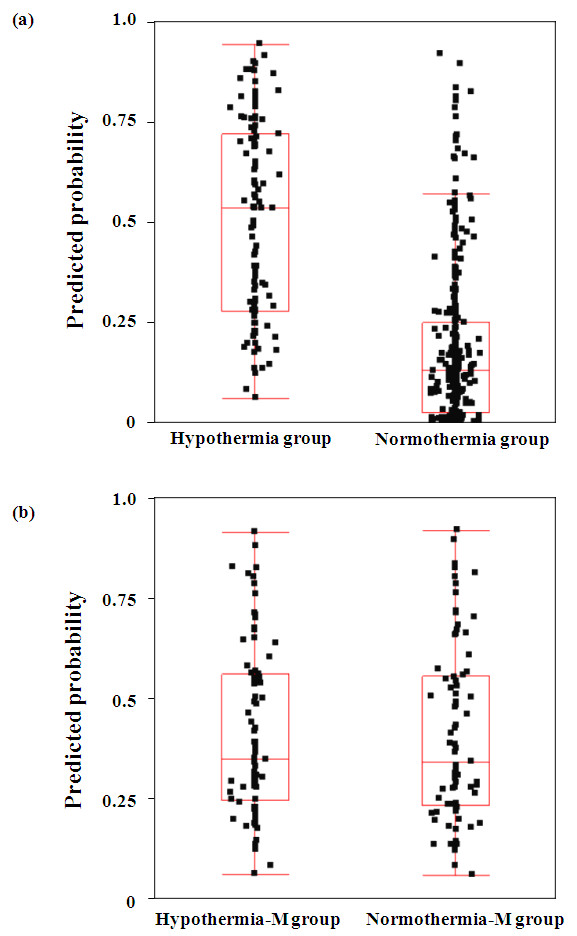
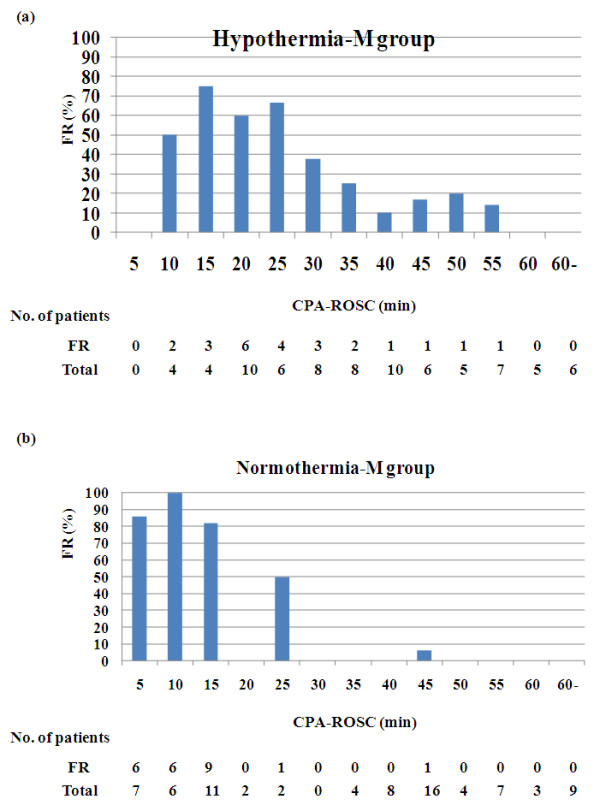
Results: The rate of favorable neurological outcome was higher (P < 0.05) in the hypothermia group (n = 110) than in the normothermia group in patients with CPA-ROSC of 15 to 20 minutes (64% vs. 17%), 20 to 25 minutes (70% vs. 8%), 25 to 30 minutes (50% vs. 7%), 35 to 40 minutes (27% vs. 0%) and 40 to 45 minutes (29% vs. 2%). A similar association was observed in a propensity-matched cohort, but the differences were not significant. There was no significant difference in the rate of favorable neurological outcome between the hypothermia-matched group and the normothermia-matched group. In the patients whose CPA-ROSC was greater than 15 minutes, however, the rate of favorable neurological outcome was higher in the hypothermia-matched group than in the normothermia-matched group (27% vs. 4%, P < 0.001). In multivariate analysis, the CPA-ROSC was an independent predictor of favorable neurological outcome (every 1 minute: odds ratio = 0.89, 95% confidence interval = 0.85 to 0.92, P < 0.001).
Conclusions: The CPA-ROSC is an independent predictor of neurological outcome. Therapeutic hypothermia is more beneficial in comatose survivors of cardiac arrest with CPA-ROSC greater than 15 minutes.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
