

Review
doi: 10.1102/1470-7330.2010.0025.
Treatment monitoring of paranasal sinus tumors by magnetic resonance imaging
Affiliations
- PMID: 20713318
- PMCID: PMC2943677
- DOI: 10.1102/1470-7330.2010.0025
Item in Clipboard
Review
Treatment monitoring of paranasal sinus tumors by magnetic resonance imaging
Cancer Imaging.
.
Abstract
Treatment monitoring of paranasal tumors is crucial, given the high rate of local and regional relapses that impairs the overall prognosis of patients. Magnetic resonance imaging (MRI) is the technique of choice to detect changes in the submucosa and deep spaces of the suprahyoid neck, inaccessible at clinical and endoscopic assessment. Correct interpretation of MRI requires detailed knowledge of the treatment applied and of the changes treatments are supposed to produce on macroscopic anatomy and tissue signals. Once such background of information is obtained, detection of recurrences is a less challenging task.
Figures
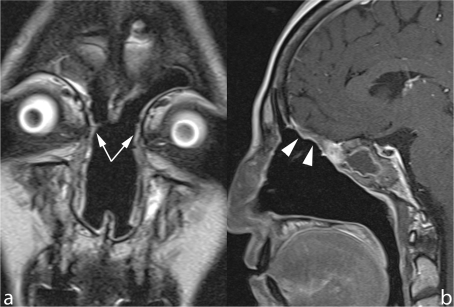
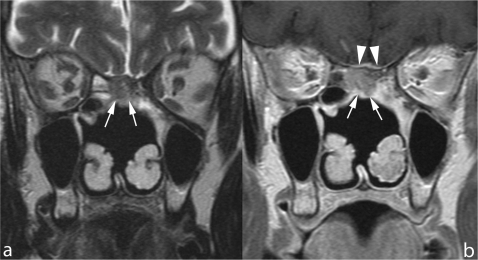
Microendoscopic ethmoidectomy and frontal sinusotomy (Draf-III approach). Coronal TSE T2 (a) and sagittal contrast enhanced SE T1 (b) show the wide communication created between frontal sinuses and nasal fossa (arrows). The duraplasty (arrowheads) exhibits a regular profile, the sphenoid sinus is occupied by thickened mucosa and retained secretions.

Follow-up scan after ethmoidectomy and craniofacial resection. Contrast-enhanced SE T1 on axial plane shows prolapse of orbital fat (arrows) into the residual nasal fossa, secondary to complete removal of the medial wall of the right orbit.
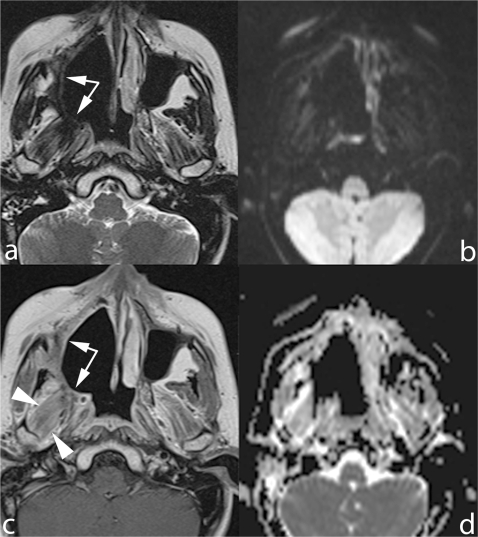
Early follow-up scan obtained after radical maxillectomy extended to the right hemipalate. The surgical cavity is delimited by a thick plaque of solid tissue (arrows) hypointense on TSE T2 (a) and mildly hyperintense on contrast-enhanced SE T1 MRI (b). This tissue is neither hyperintense DWI b-1000 (c) nor restricting on ADC map (d), thus consistent with fibrotic scar. Diffuse enhancement of lateral pterygoid muscle, secondary to post-RT inflammation (arrowheads).

Craniofacial resection performed with an open surgery approach. The meningogaleal complex exhibits mild and fairly homogeneous contrast enhancement on both SE T1 (a) and fat-saturated GE T1 (b) images, its thickness is regular all along the anteroposterior extension. Reepithelization of the surgical cavity is partially seen (arrows).
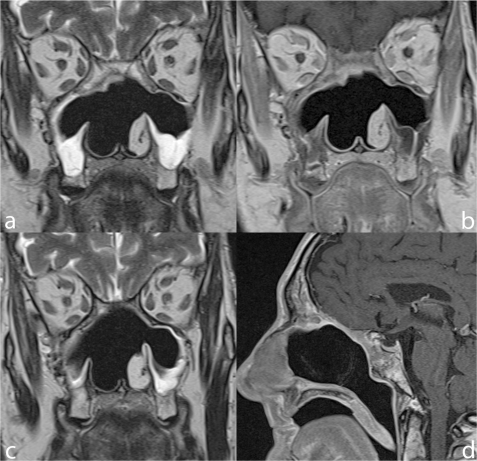
Craniofacial resection performed with the microendoscopic approach. The comparison between the scans acquired 4 months (a,b) and 20 months (c,d) after surgery demonstrates thinning of the duraplasty and nearly complete regression of mucosal thickenings.
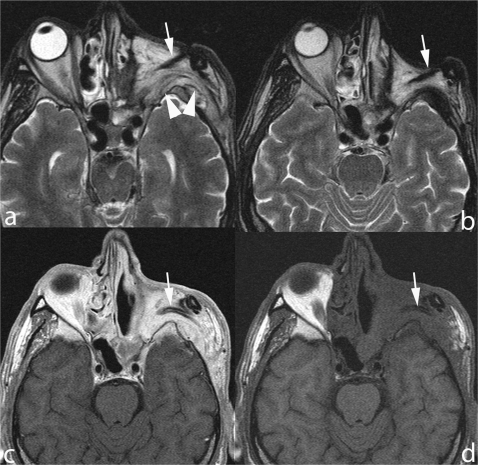
Radical ethmoidomaxillectomy with orbital exenteration and flap reconstruction. Six months after surgery (a,c,d) the flap shows a hyperintense T2 signal with diffuse and bright enhancement; these findings correspond with subacute denervation, as confirmed by the atrophy demonstrated by the MRI scan performed 12 months after surgery (b). Note the temporalis muscle tendon, rotated in the orbital cavity (arrow) and the striated appearance of muscular fibers (arrowheads), unaltered by edema.
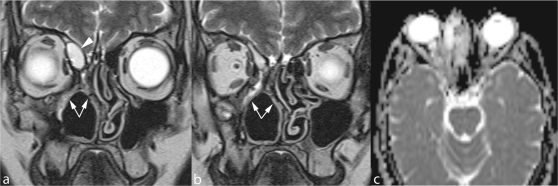
Radical ethmoidomaxillectomy. Mucosal synechiae (arrows) restrict the residual nasal fossa and obstruct frontal sinus drainage. The small expansile lesion within the lower part of the frontal sinus corresponds to a mucocele (arrowhead) that has developed within a compartmentalized cell. Absence of diffusion restriction on the ADC map (c) confirms the inflammatory nature of the expansile lesion.
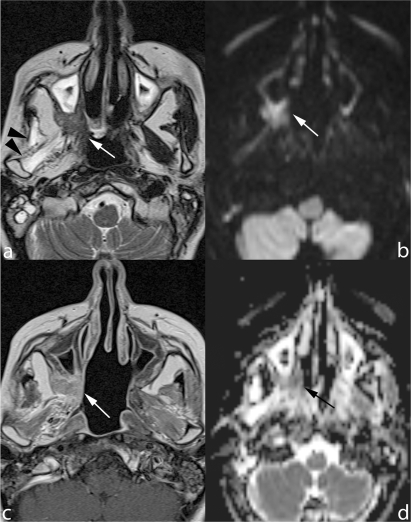
Radical maxillectomy for adenoid cystic carcinoma. A mass lesion (arrow) is seen in the lowermost part of the pterygopalatine fossa (a,b) exhibiting b-1000 hyperintensity (c) and diffusion restriction (ADC 0.98 × 10−3 mm/s) (d). Denervation atrophy of masticator muscles (arrowheads) is due to perineural spread reaching the Meckel cave and, antegradely, the mandibular nerve (not displayed in these images).
A nodule is seen at the interface between the flap filling the orbital cavity after exenteration and the skull base in a patient treated for Ewing sarcoma. Although completely unenhancing after contrast application (b), the lesion corresponds to recurrent tumor.
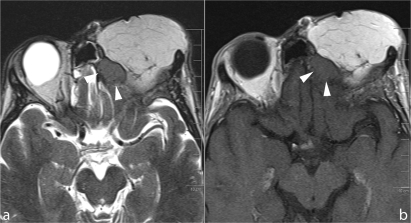
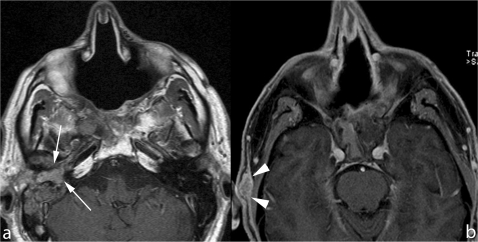
Open surgery craniofacial resection. A nodule (arrows) lies beneath the mucosa lining the surgical cavity exhibiting an intermediate T2 signal (a) and mild homogenous enhancement (b). Contact between tumor and dura of the middle cranial fossa is indirectly indicated by thickening and enhancement (arrowheads).
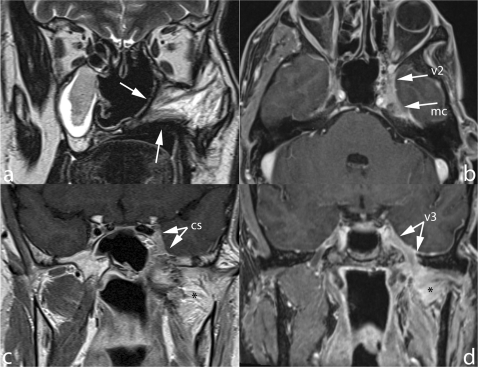
Radical maxillectomy extended to the hemipalate for squamous cell carcinoma; temporalis muscle flap reconstructs the surgical gap. Perineural recurrent tumor spreading along the maxillary nerve (v2) to reach posteriorly the cavernous sinus (cs) and Meckel cave (mc). Antegrade extension along the mandibular nerve is also seen (v3), the lateral pterygoid muscle (*) shows signs of denervation.
In two patients treated with craniofacial resection for ethmoid adenocarcinoma, follow-up MRI scans shows metastasis located, respectively, in the middle ear (arrows in (a)) and subcutaneous fat tissue (arrowheads in (b)).
References
-
- Khademi B, Moradi A, Hoseini S, Mohammadianpanah M. Malignant neoplasms of the sinonasal tract: report of 71 patients and literature review and analysis. Oral Maxillofac Surg. 2009;13:191–9. doi:10.1007/s10006-009-0170-8. PMid:19795137. - DOI - PubMed
-
- Mendenhall WM, Mendenhall CM, Riggs CE, Jr, Villaret DB, Mendenhall NP. Sinonasal undifferentiated carcinoma. Am J Clin Oncol. 2006;29:27–31. doi:10.1097/01.coc.0000189691.04140.02. PMid:16462499. - DOI - PubMed
-
- Dulguerov P, Jacobsen MS, Allal AS, Lehmann W, Calcaterra T. Nasal and paranasal sinus carcinoma: are we making progress? A series of 220 patients and a systematic review. Cancer. 2001;92:3012–29. doi:10.1002/1097-0142(20011215)92:12<3012::AID-CNCR10131>3.0.CO;2-E. - DOI - PubMed
-
- Dulguerov P, Allal AS. Nasal and paranasal sinus carcinoma: how can we continue to make progress? Curr Opin Otolaryngol Head Neck Surg. 2006;14:67–72. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical