

Hysterectomy, endometrial destruction, and levonorgestrel releasing intrauterine system (Mirena) for heavy menstrual bleeding: systematic review and meta-analysis of data from individual patients
- PMID: 20713583
- PMCID: PMC2922496
- DOI: 10.1136/bmj.c3929
Hysterectomy, endometrial destruction, and levonorgestrel releasing intrauterine system (Mirena) for heavy menstrual bleeding: systematic review and meta-analysis of data from individual patients
Abstract
Objective: To evaluate the relative effectiveness of hysterectomy, endometrial destruction (both "first generation" hysteroscopic and "second generation" non-hysteroscopic techniques), and the levonorgestrel releasing intrauterine system (Mirena) in the treatment of heavy menstrual bleeding.
Design: Meta-analysis of data from individual patients, with direct and indirect comparisons made on the primary outcome measure of patients' dissatisfaction.
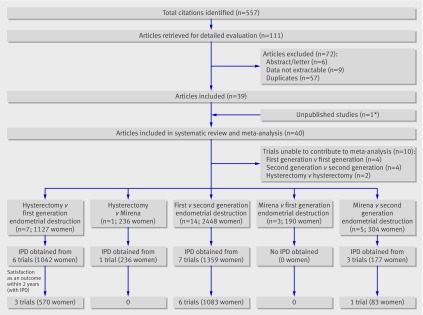
Data sources: Data were sought from the 30 randomised controlled trials identified after a comprehensive search of the Cochrane Library, Medline, Embase, and CINAHL databases, reference lists, and contact with experts. Raw data were available from 2814 women randomised into 17 trials (seven trials including 1359 women for first v second generation endometrial destruction; six trials including 1042 women for hysterectomy v first generation endometrial destruction; one trial including 236 women for hysterectomy v Mirena; three trials including 177 women for second generation endometrial destruction v Mirena). Eligibility criteria for selecting studies Randomised controlled trials comparing hysterectomy, first and second generation endometrial destruction, and Mirena for women with heavy menstrual bleeding unresponsive to other medical treatment.
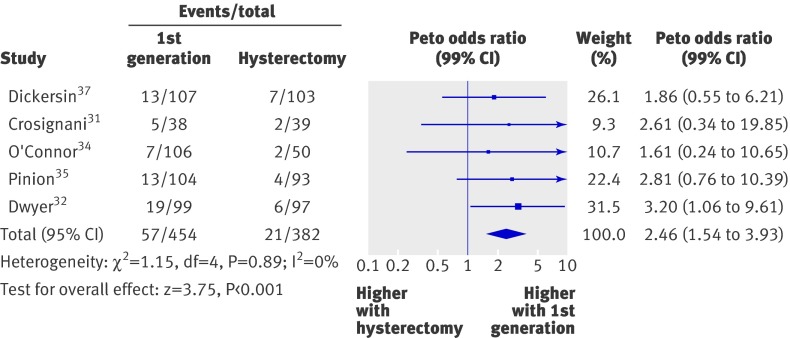
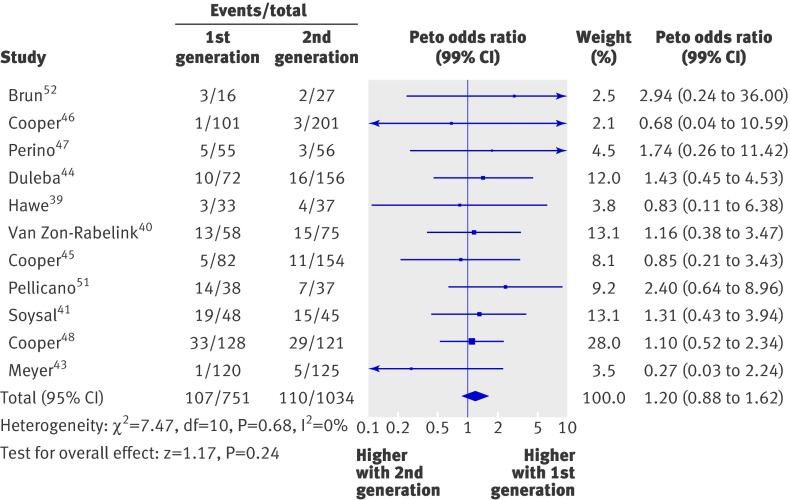
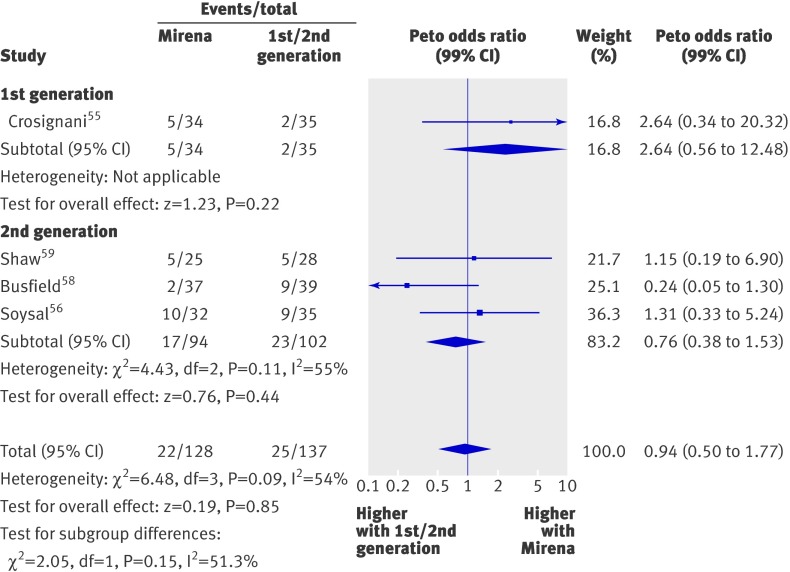
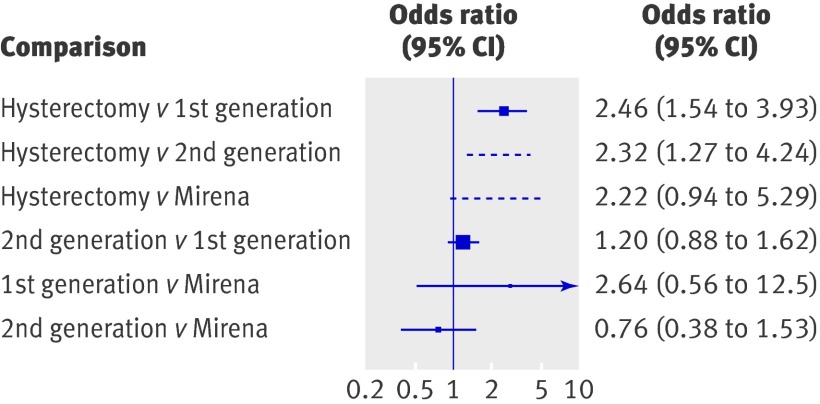
Results: At around 12 months, more women were dissatisfied with outcome with first generation hysteroscopic techniques than with hysterectomy (13% v 5%; odds ratio 2.46, 95% confidence interval 1.54 to 3.9, P<0.001), but hospital stay (weighted mean difference 3.0 days, 2.9 to 3.1 days, P<0.001) and time to resumption of normal activities (5.2 days, 4.7 to 5.7 days, P<0.001) were longer for hysterectomy. Unsatisfactory outcomes were comparable with first and second generation techniques (odds ratio 1.2, 0.9 to 1.6, P=0.2), although second generation techniques were quicker (weighted mean difference 14.5 minutes, 13.7 to 15.3 minutes, P<0.001) and women recovered sooner (0.48 days, 0.20 to 0.75 days, P<0.001), with fewer procedural complications. Indirect comparison suggested more unsatisfactory outcomes with second generation techniques than with hysterectomy (11% v 5%; odds ratio 2.3, 1.3 to 4.2, P=0.006). Similar estimates were seen when Mirena was indirectly compared with hysterectomy (17% v 5%; odds ratio 2.2, 0.9 to 5.3, P=0.07), although this comparison lacked power because of the limited amount of data available for analysis.
Conclusions: More women are dissatisfied after endometrial destruction than after hysterectomy. Dissatisfaction rates are low after all treatments, and hysterectomy is associated with increased length of stay in hospital and a longer recovery period. Definitive evidence on effectiveness of Mirena compared with more invasive procedures is lacking.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Treatment of heavy menstrual bleeding.BMJ. 2010 Aug 17;341:c3771. doi: 10.1136/bmj.c3771. BMJ. 2010. PMID: 20716600 No abstract available.
-
Hysterectomy, endometrial destruction and the levonorgestrel intrauterine system are all effective therapies for heavy menstrual bleeding; satisfaction rates are highest after hysterectomy.Evid Based Med. 2011 Apr;16(2):55-6. doi: 10.1136/ebm1168. Epub 2011 Jan 12. Evid Based Med. 2011. PMID: 21228052 No abstract available.
References
-
- Chapple A. Menorrhagia: women’s perceptions of this condition and its treatment. J Adv Nurs 1999;29:1500-6. - PubMed
-
- Prentice A. Health care implications of dysfunctional uterine bleeding. Baillieres Best Pract Res Clin Obstet Gynaecol 1999;13:181-8. - PubMed
-
- Maresh MJA, Metcalfe MA, McPherson K, Overton C, Hall V, Hargreaves J. The VALUE national hysterectomy study: description of the patients and their surgery. Br J Obstet Gynaecol 2002;109:302-12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical