

Pancreatic duct stenosis secondary to small endocrine neoplasms: a manifestation of serotonin production?
- PMID: 20713615
- PMCID: PMC2941724
- DOI: 10.1148/radiol.10100046
Pancreatic duct stenosis secondary to small endocrine neoplasms: a manifestation of serotonin production?
Abstract
Purpose: To determine if serotonin production by pancreatic endocrine neoplasms is associated with the pancreatic duct stenosis seen in patients with stenosis that is out of proportion to the size of the tumors seen on computed tomographic images.
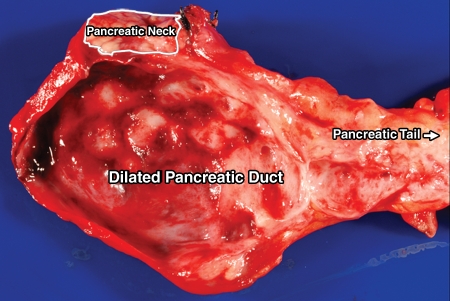
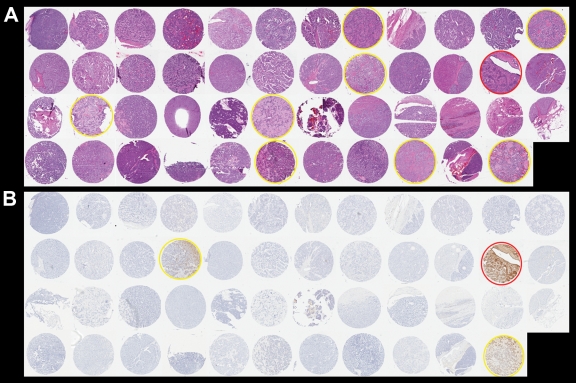
Materials and methods: Institutional approval was obtained for this HIPAA-compliant study. Informed consent was waived. Clinical and radiologic findings in six patients were reviewed. Gross and histologic findings in the resected pancreata were also assessed. Formalin-fixed paraffin-embedded tumor sections were immunolabeled with antibodies to serotonin. Tissue microarrays constructed from 47 pancreatic endocrine neoplasms from the institutional tissue bank served as controls. Histologic and serotonin immunoreactivity findings were compared between the two groups. The Fisher exact test was used to compare serotonin immunoreactivity.
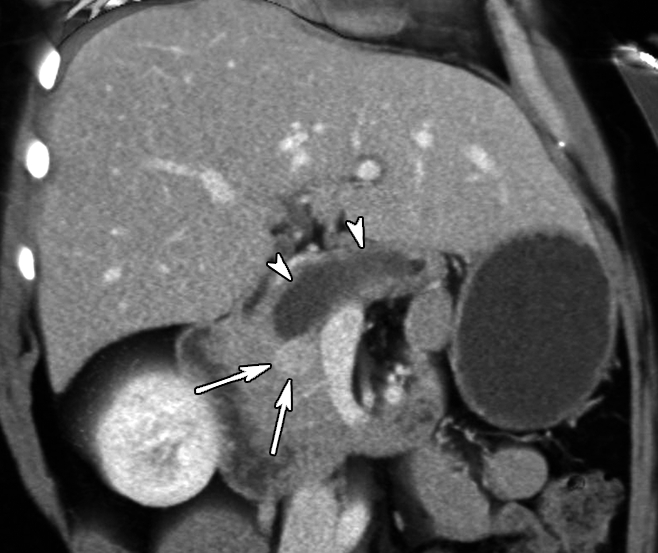
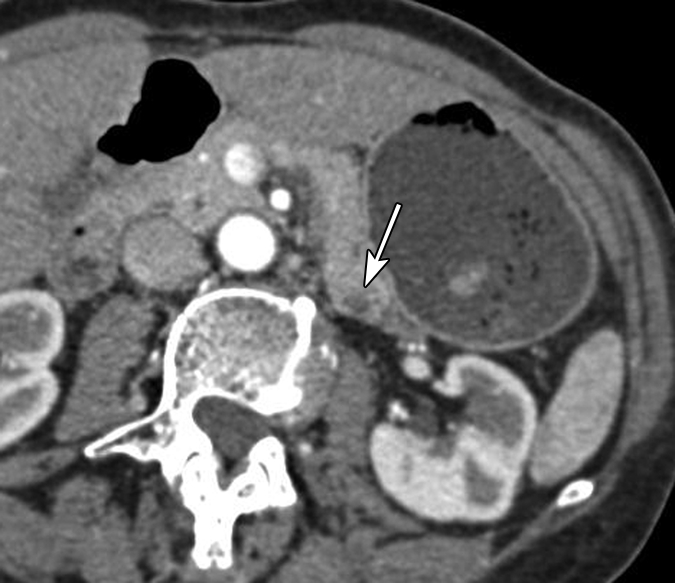
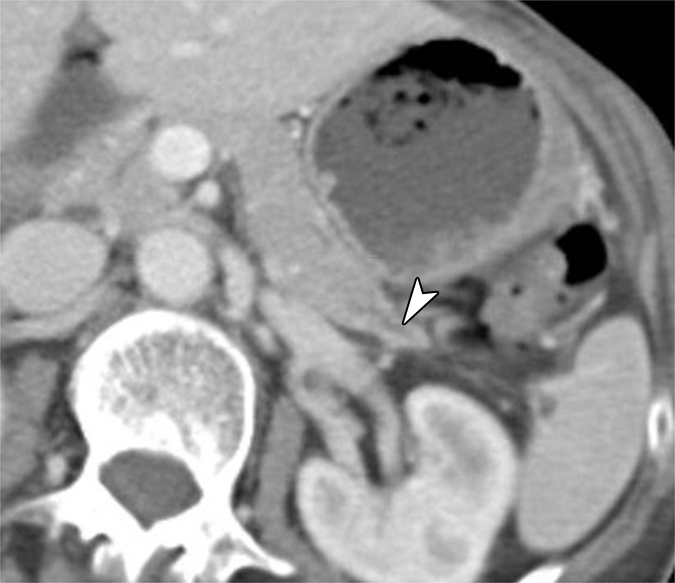
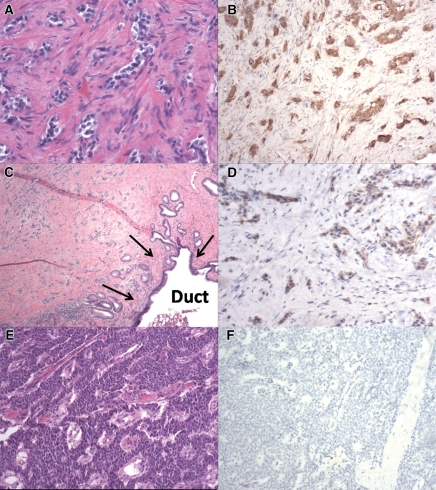
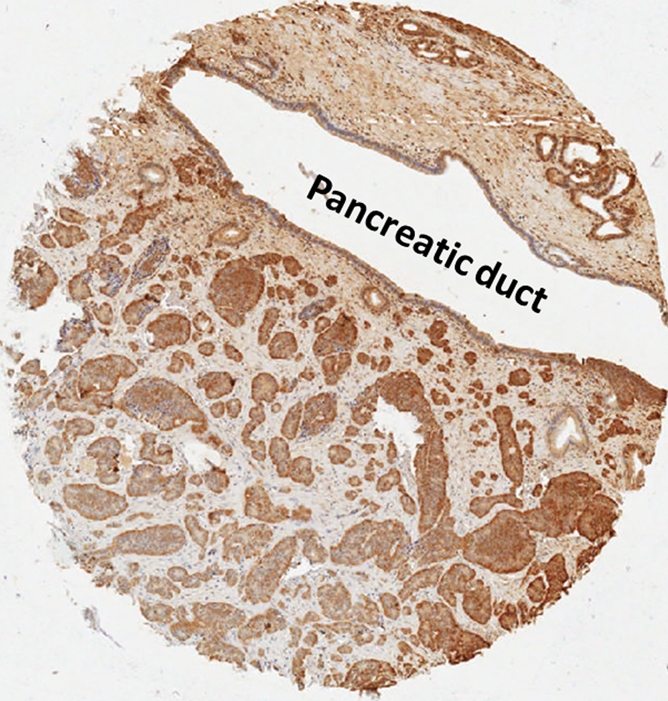
Results: Only one of the six study patients had a large dominant tumor (4 cm in the pancreatic head). All others were 2.5 cm or smaller. Four of the six pancreatic endocrine neoplasms with associated pancreatic duct stricture had prominent stromal fibrosis. Serotonin immunoreactivity was present in five (83%) patients, and this labeling was strong and diffuse in the four patients with prominent fibrosis. By contrast, stromal fibrosis was minimal in the nonimmunoreactive case. Only three (6%) of the 47 control pancreatic endocrine neoplasms were immunoreactive for serotonin (P < .01, Fisher exact test).
Conclusion: These data suggest that serotonin produced by pancreatic endocrine neoplasms may be associated with local fibrosis and stenosis of the pancreatic duct. Clinicians should be aware that small pancreatic endocrine neoplasms can produce pancreatic duct stenosis resulting in ductal dilatation and/or upstream pancreatic atrophy out of proportion to the size of the tumor.
Conflict of interest statement
Authors stated no financial relationship to disclose.
Figures




Similar articles
-
Small serotonin-producing neuroendocrine tumor of the pancreas associated with pancreatic duct obstruction.AJR Am J Roentgenol. 2011 Sep;197(3):W482-8. doi: 10.2214/AJR.10.5428. AJR Am J Roentgenol. 2011. PMID: 21862776
-
Chronic obstructive pancreatitis, nesidioblastosis, and small endocrine pancreatic tumor.Dig Dis Sci. 1987 Jul;32(7):770-4. doi: 10.1007/BF01296146. Dig Dis Sci. 1987. PMID: 3595391
-
Percutaneous fine-needle aspiration cytologic study of main pancreatic duct stenosis under pancreatographic guidance.Cancer. 1991 May 1;67(9):2395-400. doi: 10.1002/1097-0142(19910501)67:9<2395::aid-cncr2820670929>3.0.co;2-d. Cancer. 1991. PMID: 2013042
-
Assessment of pancreatic duct strictures.Gastrointest Endosc Clin N Am. 1995 Jan;5(1):125-43. Gastrointest Endosc Clin N Am. 1995. PMID: 7728341 Review.
-
[A Case of Non-Functioning Pancreatic Neuroendocrine Tumor Accompanied by Stenosis of the Main Pancreatic Duct].Gan To Kagaku Ryoho. 2017 Nov;44(12):1632-1634. Gan To Kagaku Ryoho. 2017. PMID: 29394725 Review. Japanese.
Cited by
-
Pancreatic endocrine tumors.N Am J Med Sci. 2011 Apr;3(4):164-6. doi: 10.4297/najms.2011.3164. N Am J Med Sci. 2011. PMID: 22540085 Free PMC article.
-
Pancreatic neuroendocrine tumor with stenosis of the main pancreatic duct leading to pancreatic pleural effusion: a case report.Surg Case Rep. 2020 Sep 25;6(1):222. doi: 10.1186/s40792-020-00987-7. Surg Case Rep. 2020. PMID: 32975612 Free PMC article.
-
Prognostic Features in Surgically Resected Well-Differentiated Pancreatic Neuroendocrine Tumors: An Analysis of 904 Patients with 7882 Person-Years of Follow-Up.medRxiv [Preprint]. 2025 Apr 3:2025.04.01.25325055. doi: 10.1101/2025.04.01.25325055. medRxiv. 2025. Update in: Endocr Pathol. 2025 Jun 27;36(1):24. doi: 10.1007/s12022-025-09866-z. PMID: 40236435 Free PMC article. Updated. Preprint.
-
Small serotonin-positive pancreatic endocrine tumors caused obstruction of the main pancreatic duct.World J Gastroenterol. 2012 Dec 7;18(45):6669-73. doi: 10.3748/wjg.v18.i45.6669. World J Gastroenterol. 2012. PMID: 23236243 Free PMC article.
-
Differentiation of atypical pancreatic neuroendocrine tumors from pancreatic ductal adenocarcinomas: Using whole-tumor CT texture analysis as quantitative biomarkers.Cancer Med. 2018 Oct;7(10):4924-4931. doi: 10.1002/cam4.1746. Epub 2018 Aug 27. Cancer Med. 2018. PMID: 30151864 Free PMC article.
References
-
- Jensen RT. Pancreatic neuroendocrine tumors: overview of recent advances and diagnosis. J Gastrointest Surg 2006;10(3):324–326 - PubMed
-
- Capelli P, Martignoni G, Pedica F, et al. Endocrine neoplasms of the pancreas: pathologic and genetic features. Arch Pathol Lab Med 2009;133(3):350–364 - PubMed
-
- Klöppel G, Perren A, Heitz PU. The gastroenteropancreatic neuroendocrine cell system and its tumors: the WHO classification. Ann N Y Acad Sci 2004;1014:13–27 - PubMed
-
- Horton KM, Hruban RH, Yeo C, Fishman EK. Multi-detector row CT of pancreatic islet cell tumors. RadioGraphics 2006;26(2):453–464 - PubMed
-
- Druce M, Rockall A, Grossman AB. Fibrosis and carcinoid syndrome: from causation to future therapy. Nat Rev Endocrinol 2009;5(5):276–283 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
