

Treatment of oroantral fistula with autologous bone graft and application of a non-reabsorbable membrane
- PMID: 20714437
- PMCID: PMC2920572
- DOI: 10.7150/ijms.7.267
Treatment of oroantral fistula with autologous bone graft and application of a non-reabsorbable membrane
Abstract
Aim: The aim of the current report is to illustrate an alternative technique for the treatment of oroantral fistula (OAF), using an autologous bone graft integrated by xenologous particulate bone graft.
Background: Acute and chronic oroantral communications (OAC, OAF) can occur as a result of inadequate treatment. In fact surgical procedures into the maxillary posterior area can lead to inadvertent communication with the maxillary sinus. Spontaneous healing can occur in defects smaller than 3 mm while larger communications should be treated without delay, in order to avoid sinusitis. The most used techniques for the treatment of OAF involve buccal flap, palatal rotation - advancement flap, Bichat fat pad. All these surgical procedures are connected with a significant risk of morbidity of the donor site, infections, avascular flap necrosis, impossibility to repeat the surgical technique after clinical failure, and patient discomfort.
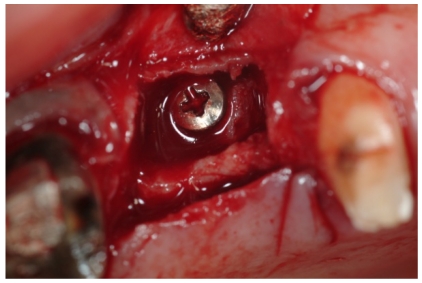
Case presentation: We report a 65-years-old female patient who came to our attention for the presence of an OAF and was treated using an autologous bone graft integrated by xenologous particulate bone graft. An expanded polytetrafluoroethylene titanium-reinforced membrane (Gore-Tex) was used in order to obtain an optimal reconstruction of soft tissues and to assure the preservation of the bone graft from epithelial connection.
Conclusions: This surgical procedure showed a good stability of the bone grafts, with a complete resolution of the OAF, optimal management of complications, including patient discomfort, and good regeneration of soft tissues.
Clinical significance: The principal advantage of the use of autologous bone graft with an expanded polytetrafluoroethylene titanium-reinforced membrane (Gore-Tex) to guide the bone regeneration is that it assures a predictable healing and allows a possible following implant-prosthetic rehabilitation.
Keywords: bone regeneration; maxillary sinus.; oroantral fistula.
Conflict of interest statement
Competing interests: The authors declare that they have no competing interests.
Figures










References
-
- Punwutikorn J, Waikakul A, Pairuchvej V. Clinically significant oroantral communications—a study of incidence and site. Int J Oral Maxillofac Surg. 1994;23:19–21. - PubMed
-
- Haas R, Watzak G, Baron M, Tepper G, Mailath G, Watzek G. A preliminary study of monocortical bone grafts for oroantral fistula closure. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003 Sep;96(3):263–6. - PubMed
-
- Lee BK. One-stage operation of large oroantral fistula closure, sinus lifting, and autogenous bone grafting for dental implant installation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:707–13. - PubMed
-
- Hauman CH, Chandler NP, Tong DC. Endodontic implications of the maxillary sinus: a review. Int Endod J. 2002 Feb;35(2):127–141. - PubMed
-
- Waldrop TC, Semba SE. Closure of oroantral communication using guided tissue regeneration and an absorbable gelatin membrane. J Periodontol. 1993 Nov;64(11):1061–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
