

Colostomy closure: how to avoid complications
- PMID: 20714731
- PMCID: PMC2962784
- DOI: 10.1007/s00383-010-2690-6
Colostomy closure: how to avoid complications
Abstract
Purpose: Colostomy is an operation frequently performed in pediatric surgery. Despite its benefits, it can produce significant morbidity. In a previous publication we presented our experience with the errors and complications that occurred during cases of colostomy creation. We now have focused in the morbidity related to the colostomy closure. The technical details that might have contributed to the minimal morbidity we experienced are described.
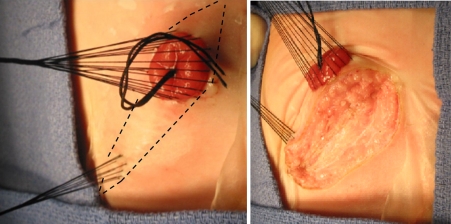
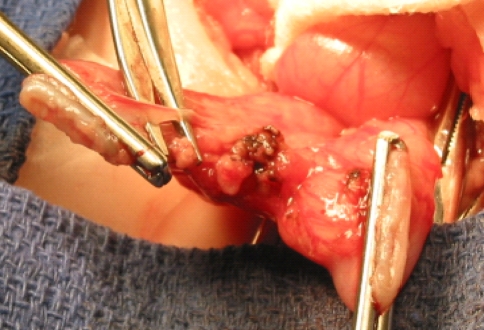
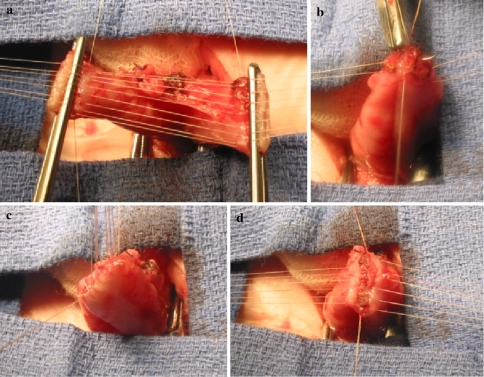
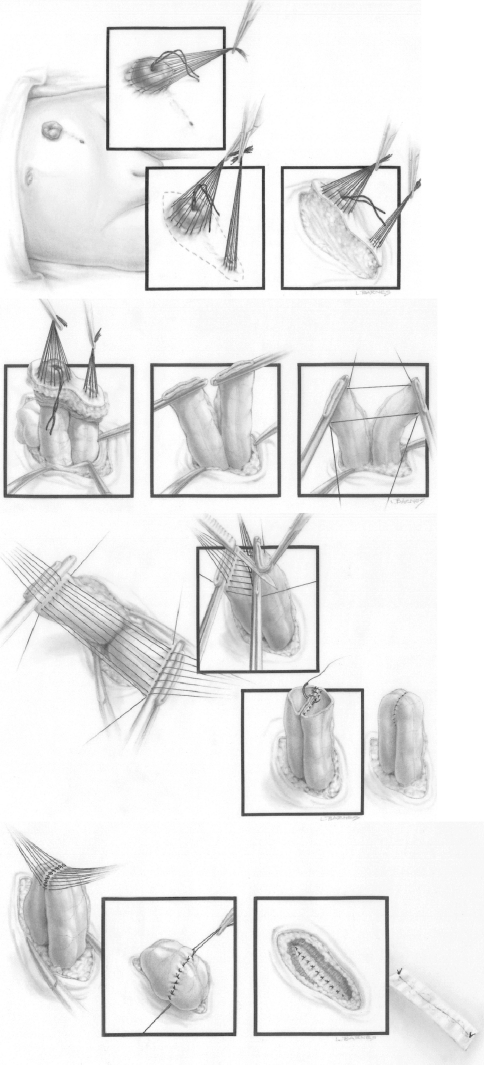
Methods: The medical records of 649 patients who underwent colostomy closure over a 28-year period were retrospectively reviewed looking for complications following these procedures. Our perioperative protocol for colostomy closure consisted in: clear fluids by mouth and repeated proximal stoma irrigations 24 h prior to the operation. Administration of IV antibiotics during anesthesia induction and continued for 48 h. Meticulous surgical technique that included: packing of the proximal stoma, plastic drape to immobilize the surgical field, careful hemostasis, emphasis in avoiding contamination, cleaning the edge of the stomas to allow a good 2-layer, end-to-end anastomosis with separated long-term absorbable sutures, generous irrigation of the peritoneal cavity and subsequent layers with saline solution, closure by layers to avoid dead space, and avoidance of hematomas. No drains and no nasogastric tubes were used. Oral fluids were started the day after surgery and patients were discharged 48-72 h after the operation.
Results: The original diagnoses of the patients were: anorectal malformation (583), Hirschsprung's disease (53), and others (13). 10 patients (1.5%) had complications: 6 had intestinal obstruction (5 due to small bowel adhesions, 1 had temporary delay of the function of the anastomosis due to a severe size discrepancy between proximal and distal stoma with a distal microcolon) and 4 incisional hernias. There were no anastomotic dehiscences or wound infection. There was no bleeding, no anastomotic stricture and no mortality.
Conclusion: Based on this experience we believe that colostomy closure can be performed with minimal morbidity provided a meticulous technique is observed.
Figures


References
-
- Kiely EM, Sparnon AL. Stoma closure in infants and children. Pediatr Surg Int. 1987;2:95–97.
-
- Millar AJK, Lakhoo K, Rode H, et al. Bowel stomas in infants and children. A 5-year audit of 203 patients. S Afr J Surg. 1993;3:110–113. - PubMed
-
- Rees BI, Thomas DFM, Negam M. Colostomies in infancy and childhood. Z Kinderchir. 1982;36:100–102. - PubMed
-
- Mollitt DL, Malangoni MA, Ballantine TVN, et al. Colostomy complications in children. An analysis of 146 cases. Arch Surg. 1980;115:445–458. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
