

Tumor infiltration by FcγRIII (CD16)+ myeloid cells is associated with improved survival in patients with colorectal carcinoma
- PMID: 20715106
- PMCID: PMC3426287
- DOI: 10.1002/ijc.25609
Tumor infiltration by FcγRIII (CD16)+ myeloid cells is associated with improved survival in patients with colorectal carcinoma
Abstract
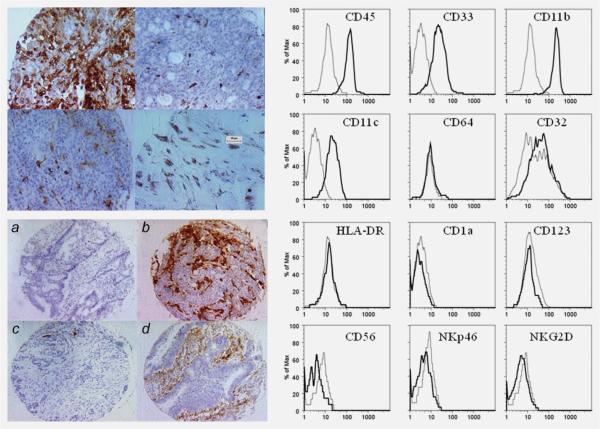
The prognostic significance of macrophage and natural killer (NK) cell infiltration in colorectal carcinoma (CRC) microenvironment is unclear. We investigated the CRC innate inflammatory infiltrate in over 1,600 CRC using two independent tissue microarrays and immunohistochemistry. Survival time was assessed using the Kaplan-Meier method and Cox proportional hazards regression analysis in a multivariable setting. Spearman's rank correlation tested the association between macrophage and lymphocyte infiltration. The Basel study included over 1,400 CRCs. The level of CD16+ cell infiltration correlated with that of CD3+ and CD8+ lymphocytes but not with NK cell infiltration. Patients with high CD16+ cell infiltration (score 2) survived longer than patients with low (score 1) infiltration (p = 0.008), while no survival difference between patients with score 1 or 2 for CD56+ (p = 0.264) or CD57+ cell (p = 0.583) infiltration was detected. CD16+ infiltrate was associated with improved survival even after adjusting for known prognostic factors including pT, pN, grade, vascular invasion, tumor growth and age [(p = 0.001: HR (95% CI) = 0.71 (0.6-0.9)]. These effects were independent from CD8+ lymphocyte infiltration [(p = 0.036: HR (95% CI) = 0.81 (0.7-0.9)] and presence of metastases [(p = 0.002: HR (95% CI) = 0.43 (0.3-0.7)]. Phenotypic studies identified CD16+ as CD45+CD33+CD11b+CD11c+ but CD64- HLA-DR-myeloid cells. Beneficial effects of CD16+ cell infiltration were independently validated by a study carried out at the University of Athens confirming that patients with CD16 score 2 survived longer than patients with score 1 CRCs (p = 0.011). Thus, CD16+ cell infiltration represents a novel favorable prognostic factor in CRC.
Copyright © 2010 UICC.
Figures


References
-
- Mamounas E, Wieand S, Wolmark N, Bear HD, Atkins JN, Song K, Jones J, Rockette H. Comparative efficacy of adjuvant chemotherapy in patients with Dukes' B versus Dukes' C colon cancer: results from four National Surgical Adjuvant Breast and Bowel Project adjuvant studies (C-01, C-02, C-03, and C-04) J Clin Oncol. 1999;17:1349–55. - PubMed
-
- Allegra CJ, Jessup JM, Somerfield MR, Hamilton SR, Hammond EH, Hayes DF, McAllister PK, Morton RF, Schilsky RL. American Society of Clinical Oncology provisional clinical opinion: testing for KRAS gene mutations in patients with metastatic colorectal carcinoma to predict response to anti-epidermal growth factor receptor monoclonal antibody therapy. J Clin Oncol. 2009;27:2091–6. - PubMed
-
- Galon J, Costes A, Sanchez-Cabo F, Kirilovsky A, Mlecnik B, Lagorce-Pages C, Tosolini M, Camus M, Berger A, Wind P, Zinzindohoue F, Bruneval P, et al. Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science. 2006;313:1960–4. - PubMed
-
- Galon J, Fridman WH, Pages F. The adaptive immunologic microenvironment in colorectal cancer: a novel perspective. Cancer Res. 2007;67:1883–6. - PubMed
-
- Pages F, Berger A, Camus M, Sanchez-Cabo F, Costes A, Molidor R, Mlecnik B, Kirilovsky A, Nilsson M, Damotte D, Meatchi T, Bruneval P, et al. Effector memory T cells, early metastasis, and survival in colorectal cancer. N Engl J Med. 2005;353:2654–66. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
