

Max CAPR: high-resolution 3D contrast-enhanced MR angiography with acquisition times under 5 seconds
- PMID: 20715291
- PMCID: PMC3086564
- DOI: 10.1002/mrm.22434
Max CAPR: high-resolution 3D contrast-enhanced MR angiography with acquisition times under 5 seconds
Abstract
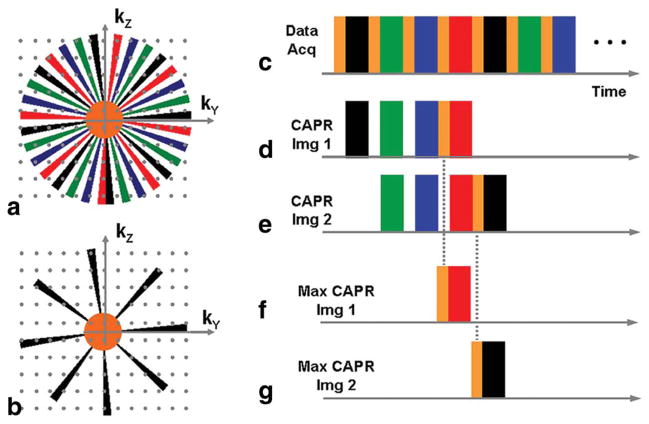
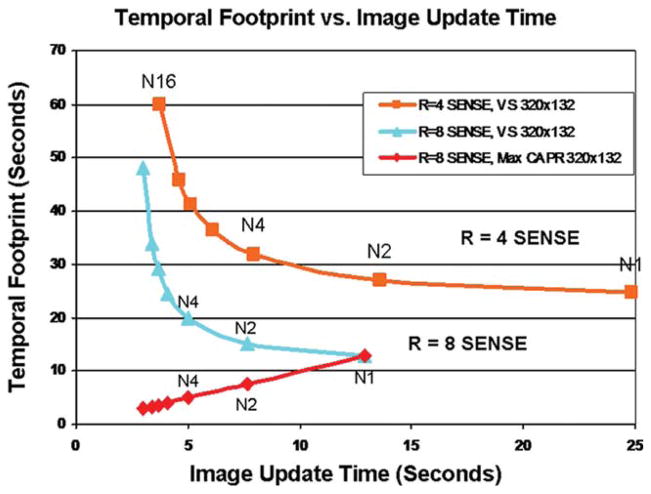
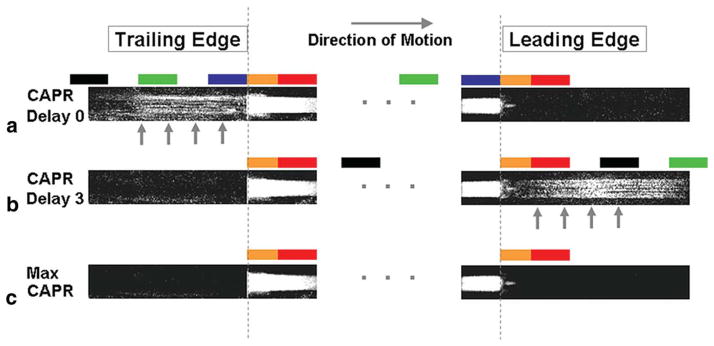
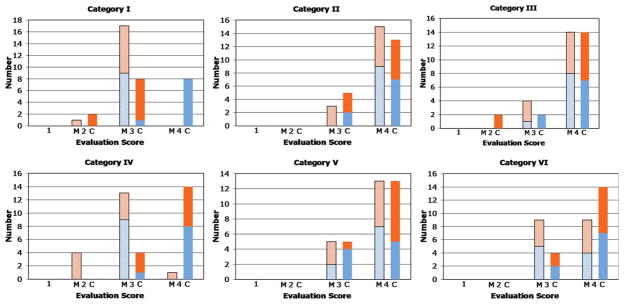
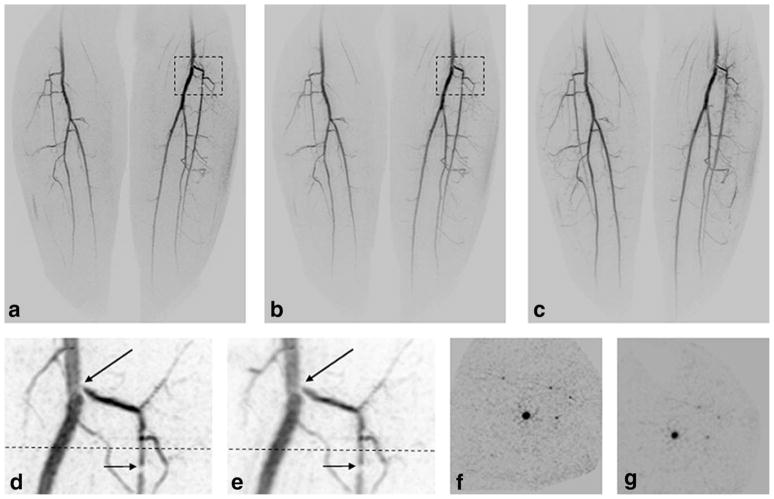
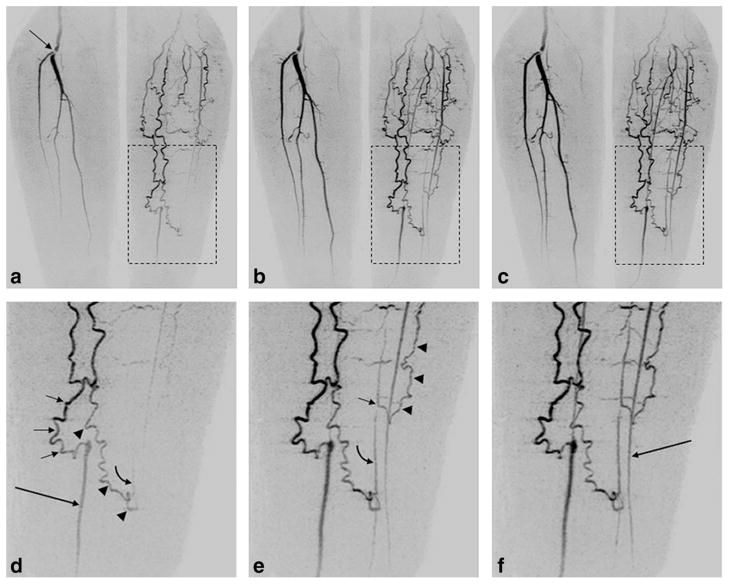
High temporal and spatial resolution is desired in imaging of vascular abnormalities having short arterial-to-venous transit times. Methods that exploit temporal correlation to reduce the observed frame time demonstrate temporal blurring, obfuscating bolus dynamics. Previously, a Cartesian acquisition with projection reconstruction-like (CAPR) sampling method has been demonstrated for three-dimensional contrast-enhanced angiographic imaging of the lower legs using two-dimensional sensitivity-encoding acceleration and partial Fourier acceleration, providing 1mm isotropic resolution of the calves, with 4.9-sec frame time and 17.6-sec temporal footprint. In this work, the CAPR acquisition is further undersampled to provide a net acceleration approaching 40 by eliminating all view sharing. The tradeoff of frame time and temporal footprint in view sharing is presented and characterized in phantom experiments. It is shown that the resultant 4.9-sec acquisition time, three-dimensional images sets have sufficient spatial and temporal resolution to clearly portray arterial and venous phases of contrast passage. It is further hypothesized that these short temporal footprint sequences provide diagnostic quality images. This is tested and shown in a series of nine contrast-enhanced MR angiography patient studies performed with the new method.
Figures


Similar articles
-
Acceleration apportionment: a method of improved 2D SENSE acceleration applied to 3D contrast-enhanced MR angiography.Magn Reson Med. 2014 Feb;71(2):672-80. doi: 10.1002/mrm.24700. Magn Reson Med. 2014. PMID: 23450817 Free PMC article.
-
Interleaved variable density sampling with a constrained parallel imaging reconstruction for dynamic contrast-enhanced MR angiography.Magn Reson Med. 2011 Aug;66(2):428-36. doi: 10.1002/mrm.22814. Epub 2011 Feb 28. Magn Reson Med. 2011. PMID: 21360740 Free PMC article.
-
High spatial and temporal resolution imaging of the arterial vasculature of the lower extremity with contrast enhanced MR angiography.Clin Anat. 2011 May;24(4):478-88. doi: 10.1002/ca.21124. Epub 2011 Jan 12. Clin Anat. 2011. PMID: 21509813 Free PMC article.
-
Highly undersampled contrast-enhanced MRA with iterative reconstruction: Integration in a clinical setting.Magn Reson Med. 2015 Dec;74(6):1652-60. doi: 10.1002/mrm.25565. Epub 2014 Dec 17. Magn Reson Med. 2015. PMID: 25522299
-
High temporal and spatial resolution 3D time-resolved contrast-enhanced magnetic resonance angiography of the hands and feet.J Magn Reson Imaging. 2011 Jul;34(1):2-12. doi: 10.1002/jmri.22469. J Magn Reson Imaging. 2011. PMID: 21698702 Free PMC article. Review.
Cited by
-
Non-Cartesian parallel imaging reconstruction.J Magn Reson Imaging. 2014 Nov;40(5):1022-40. doi: 10.1002/jmri.24521. Epub 2014 Jan 10. J Magn Reson Imaging. 2014. PMID: 24408499 Free PMC article. Review.
-
Sparse-CAPR: highly accelerated 4D CE-MRA with parallel imaging and nonconvex compressive sensing.Magn Reson Med. 2011 Oct;66(4):1019-32. doi: 10.1002/mrm.22892. Epub 2011 May 23. Magn Reson Med. 2011. PMID: 21608028 Free PMC article.
-
Rapid time-resolved magnetic resonance angiography via a multiecho radial trajectory and GraDeS reconstruction.Magn Reson Med. 2013 Feb;69(2):346-59. doi: 10.1002/mrm.24256. Epub 2012 Apr 3. Magn Reson Med. 2013. PMID: 22473742 Free PMC article.
-
Time-resolved bolus-chase MR angiography with real-time triggering of table motion.Magn Reson Med. 2010 Sep;64(3):629-37. doi: 10.1002/mrm.22537. Magn Reson Med. 2010. PMID: 20597121 Free PMC article.
-
Noncontrast-enhanced three-dimensional (3D) intracranial MR angiography using pseudocontinuous arterial spin labeling and accelerated 3D radial acquisition.Magn Reson Med. 2013 Mar 1;69(3):708-15. doi: 10.1002/mrm.24298. Epub 2012 Apr 24. Magn Reson Med. 2013. PMID: 22532423 Free PMC article.
References
-
- Prince MR, Yucel EK, Kaufman JA, Harrison DC, Geller SC. Dynamic gadolinium-enhanced three-dimensional abdominal MR arteriography. J Magn Reson Imaging. 1993;3:877–881. - PubMed
-
- Zhang H, Maki JH, Prince MR. 3D contrast-enhanced MR angiography. J Magn Reson Imaging. 2007;25:13–25. - PubMed
-
- Wilman AH, Riederer SJ, King BF, Debbins JP, Rossman PJ, Ehman RL. Fluoroscopically triggered contrast-enhanced three-dimensional MR angiography with elliptical centric view order: application to the renal arteries. Radiology. 1997;205:137–146. - PubMed
-
- Huston J, 3rd, Fain SB, Riederer SJ, Wilman AH, Bernstein MA, Busse RF. Carotid arteries: maximizing arterial to venous contrast in fluoroscopically triggered contrast-enhanced MR angiography with elliptic centric view ordering. Radiology. 1999;211:265–273. - PubMed
-
- Wang Y, Johnston DL, Breen JF, Huston J, 3rd, Jack CR, Julsrud PR, Kiely MJ, King BF, Riederer SL, Ehman RL. Dynamic MR digital subtraction angiography using contrast enhancement, fast data acquisition, and complex subtraction. Magn Reson Med. 1996;36:551–556. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
