

Effects of intensive repetition of a new facilitation technique on motor functional recovery of the hemiplegic upper limb and hand
- PMID: 20715890
- PMCID: PMC2942772
- DOI: 10.3109/02699052.2010.506855
Effects of intensive repetition of a new facilitation technique on motor functional recovery of the hemiplegic upper limb and hand
Abstract
Objective: To study the effects on the hemiplegic upper limb of repetitive facilitation exercises (RFEs) using a novel facilitation technique, in which the patient's intention to move the hemiplegic upper limb or finger was followed by realization of the movement using multiple sensory stimulations.
Methods: Twenty-three stroke patients were enrolled in a cross-over study in which 2-week RFE sessions (100 repetitions each of five-to-eight types of facilitation exercise per day) were alternated with 2-week conventional rehabilitation (CR) sessions, for a total of four sessions. Treatments were begun with the 2-week RFE session in one group and the 2-week CR session in the second group.
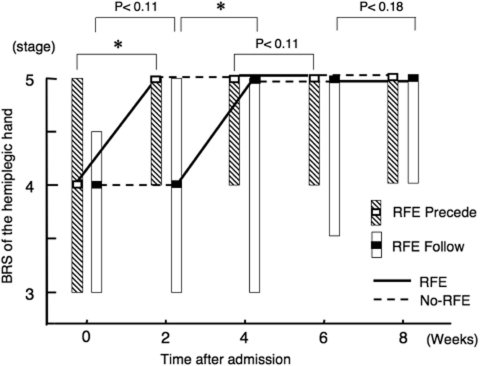
Results: After the first 2-week RFE session, both groups showed improvements in the Brunnstrom stages of the upper limb and the hand, in contrast to the small improvements observed during the first CR session. The Simple Test for Evaluating Hand Function (STEF) score, which evaluates the ability of manipulating objects, in both groups improved during both sessions. After the second 2-week RFE and CR sessions, both groups showed little further improvement except in the STEF score.
Conclusion: The novel RFEs promoted the functional recovery of the hemiplegic upper limb and hand to a greater extent than the CR sessions.
Figures






Similar articles
-
Addition of intensive repetition of facilitation exercise to multidisciplinary rehabilitation promotes motor functional recovery of the hemiplegic lower limb.J Rehabil Med. 2004 Jul;36(4):159-64. doi: 10.1080/16501970410029753. J Rehabil Med. 2004. PMID: 15370731 Clinical Trial.
-
Effects of repetitive trascranial magnetic stimulation on repetitive facilitation exercises of the hemiplegic hand in chronic stroke patients.J Rehabil Med. 2013 Sep;45(9):843-7. doi: 10.2340/16501977-1175. J Rehabil Med. 2013. PMID: 23817976 Clinical Trial.
-
Robotic-assisted rehabilitation of the upper limb after acute stroke.Arch Phys Med Rehabil. 2007 Feb;88(2):142-9. doi: 10.1016/j.apmr.2006.10.032. Arch Phys Med Rehabil. 2007. PMID: 17270510 Clinical Trial.
-
Quantitative measurement of finger usage in stroke hemiplegia using ring-shaped wearable devices.J Neuroeng Rehabil. 2023 Jun 6;20(1):73. doi: 10.1186/s12984-023-01199-4. J Neuroeng Rehabil. 2023. PMID: 37280649 Free PMC article.
-
Effects of repetitive facilitative exercise with neuromuscular electrical stimulation, vibratory stimulation and repetitive transcranial magnetic stimulation of the hemiplegic hand in chronic stroke patients.Int J Neurosci. 2016 Nov;126(11):1007-12. doi: 10.3109/00207454.2015.1094473. Epub 2015 Oct 16. Int J Neurosci. 2016. PMID: 26473535
Cited by
-
Research on adaptive impedance control technology of upper limb rehabilitation robot based on impedance parameter prediction.Front Bioeng Biotechnol. 2024 Jan 3;11:1332689. doi: 10.3389/fbioe.2023.1332689. eCollection 2023. Front Bioeng Biotechnol. 2024. PMID: 38234302 Free PMC article.
-
Effectiveness of intelligent robotic-assisted training system combined with repetitive facilitative exercise on upper limb motor function after stroke: a randomized controlled trial.BMC Sports Sci Med Rehabil. 2025 Jul 3;17(1):178. doi: 10.1186/s13102-025-01234-y. BMC Sports Sci Med Rehabil. 2025. PMID: 40611355 Free PMC article.
-
The effect of Monkey Chair and Band exercise system on shoulder range of motion and pain in post-stroke patients with hemiplegia.J Phys Ther Sci. 2016 Aug;28(8):2232-7. doi: 10.1589/jpts.28.2232. Epub 2016 Aug 31. J Phys Ther Sci. 2016. PMID: 27630403 Free PMC article.
-
Non-noxious skin stimulation activates the nucleus basalis of Meynert and promotes NGF secretion in the parietal cortex via nicotinic ACh receptors.J Physiol Sci. 2014 Jul;64(4):253-60. doi: 10.1007/s12576-014-0313-z. Epub 2014 May 7. J Physiol Sci. 2014. PMID: 24801530 Free PMC article.
-
OpenSEA: a 3D printed planetary gear series elastic actuator for a compliant elbow joint exoskeleton.Front Robot AI. 2025 Feb 28;12:1528266. doi: 10.3389/frobt.2025.1528266. eCollection 2025. Front Robot AI. 2025. PMID: 40093856 Free PMC article.
References
-
- Kott MBS, Voss DB. New York: Harper & Row; 1956. Proprioceptive neuromuscular facilitation.
-
- Brunnstrom S. New York: Harper & Row; 1970. Movement therapy in hemiplegia: A neuro-physiological approach.
-
- Bobath B. 2nd ed. London: Heineman Medical Books; 1978. Adult hemiplegia: Evaluation and treatment.
-
- Kraft GH, Fitts SS, Hammond MC. Techniques to improve function of the arm and hand in chronic hemiplegia. Archives of Physical Medicine and Rehabilitation. 1992;73:220–227. - PubMed
-
- Lincoln NB, Parry RH, Vass CD. Randomized, controlledtrial to evaluate increased intensity of physiotherapy treatment of arm function after stroke. Stroke. 1999;30:573–579. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical