

Induction of the vascular endothelial growth factor pathway in the brain of adults with fatal falciparum malaria is a non-specific response to severe disease
- PMID: 20716170
- PMCID: PMC2941727
- DOI: 10.1111/j.1365-2559.2010.03619.x
Induction of the vascular endothelial growth factor pathway in the brain of adults with fatal falciparum malaria is a non-specific response to severe disease
Abstract
Aims: Pathological or neuroprotective mechanisms in the brain in severe malaria may arise from microvascular obstruction with malaria-parasitized erythrocytes. This study aimed to investigate the role of hypoxia and induction of the vascular endothelial growth factor (VEGF) pathway in the neuropathophysiology of severe malaria.
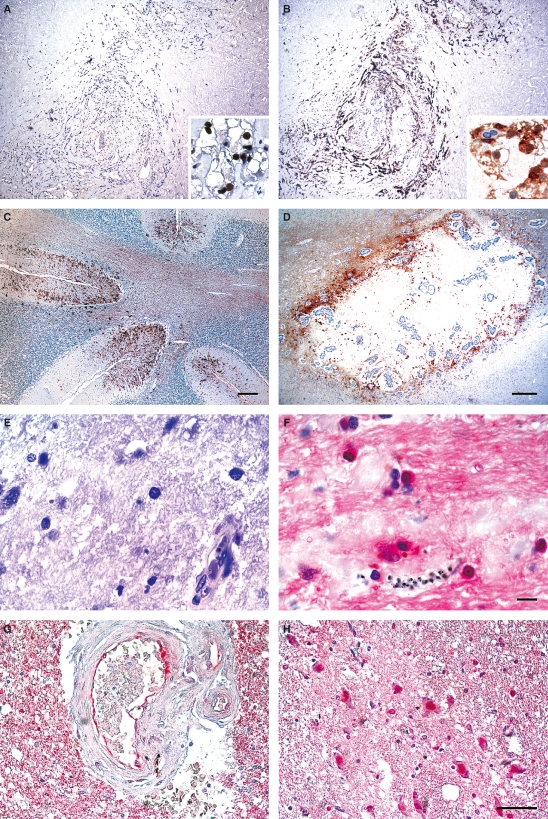
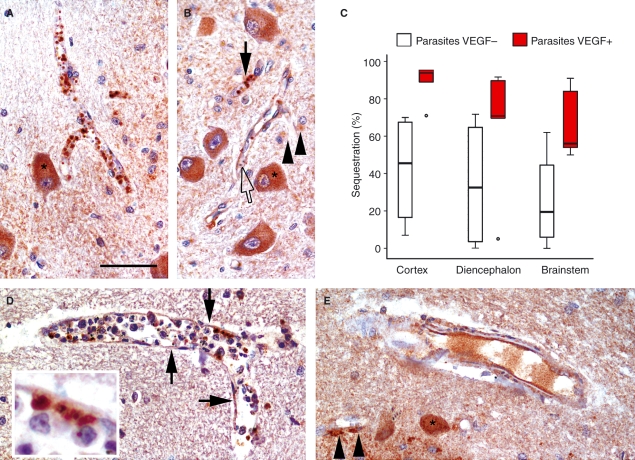
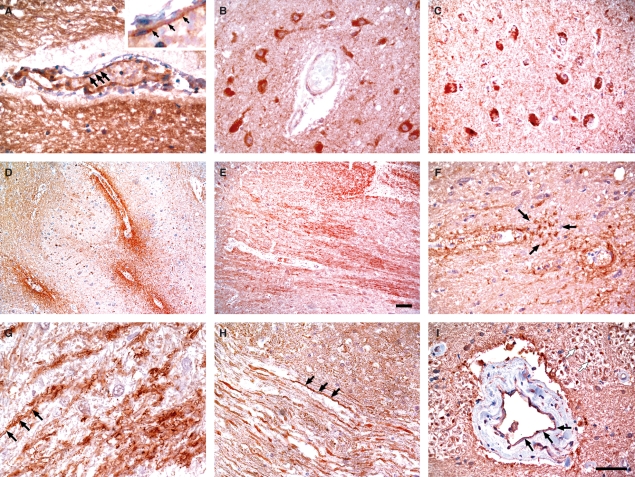
Methods and results: Immunohistochemistry was performed on post mortem brain tissue sections from 20 cases of severe malaria and examined for the expression of transcriptional regulators of VEGF [hypoxia-inducible factor-1 alpha (HIF-1alpha), HIF-2alpha], DEC-1, VEGF, VEGF receptors 1 and 2, and the activated, phosphorylated VEGF receptor 2 (pKDR). HIFs showed limited protein expression and/or translocation to cell nuclei in severe malaria, but DEC-1, which is more stable and regulated by HIF-1alpha, was observed. There was heterogeneous expression of VEGF and its receptors in severe malaria and non-malarial disease controls. pKDR expression on vessels was greater in malaria cases than in controls but did not correlate with parasite sequestration. VEGF uptake by malaria parasites was observed.
Conclusions: VEGF and its receptor expression levels in severe malaria reflect a non-specific response to severe systemic disease. Potential manipulation of events at the vasculature by the parasite requires further investigation.
Figures

Similar articles
-
Protective or pathogenic effects of vascular endothelial growth factor (VEGF) as potential biomarker in cerebral malaria.Pathog Glob Health. 2014 Mar;108(2):67-75. doi: 10.1179/2047773214Y.0000000130. Epub 2014 Mar 7. Pathog Glob Health. 2014. PMID: 24601908 Free PMC article. Review.
-
Host vascular endothelial growth factor is trophic for Plasmodium falciparum-infected red blood cells.Asian Pac J Allergy Immunol. 2008 Mar;26(1):37-45. Asian Pac J Allergy Immunol. 2008. PMID: 18595528
-
Binding Heterogeneity of Plasmodium falciparum to Engineered 3D Brain Microvessels Is Mediated by EPCR and ICAM-1.mBio. 2019 May 28;10(3):e00420-19. doi: 10.1128/mBio.00420-19. mBio. 2019. PMID: 31138740 Free PMC article.
-
Coma in fatal adult human malaria is not caused by cerebral oedema.Malar J. 2011 Sep 17;10:267. doi: 10.1186/1475-2875-10-267. Malar J. 2011. PMID: 21923924 Free PMC article.
-
A unified hypothesis for the genesis of cerebral malaria: sequestration, inflammation and hemostasis leading to microcirculatory dysfunction.Trends Parasitol. 2006 Nov;22(11):503-8. doi: 10.1016/j.pt.2006.09.002. Epub 2006 Sep 18. Trends Parasitol. 2006. PMID: 16979941 Review.
Cited by
-
Pathogenic CD8+ T Cells Cause Increased Levels of VEGF-A in Experimental Malaria-Associated Acute Respiratory Distress Syndrome, but Therapeutic VEGFR Inhibition Is Not Effective.Front Cell Infect Microbiol. 2017 Sep 20;7:416. doi: 10.3389/fcimb.2017.00416. eCollection 2017. Front Cell Infect Microbiol. 2017. PMID: 29034214 Free PMC article.
-
Systemic and Cerebral Vascular Endothelial Growth Factor Levels Increase in Murine Cerebral Malaria along with Increased Calpain and Caspase Activity and Can be Reduced by Erythropoietin Treatment.Front Immunol. 2014 Jun 19;5:291. doi: 10.3389/fimmu.2014.00291. eCollection 2014. Front Immunol. 2014. PMID: 24995009 Free PMC article.
-
CNS hypoxia is more pronounced in murine cerebral than noncerebral malaria and is reversed by erythropoietin.Am J Pathol. 2011 Oct;179(4):1939-50. doi: 10.1016/j.ajpath.2011.06.027. Epub 2011 Aug 18. Am J Pathol. 2011. PMID: 21854739 Free PMC article.
-
Protective or pathogenic effects of vascular endothelial growth factor (VEGF) as potential biomarker in cerebral malaria.Pathog Glob Health. 2014 Mar;108(2):67-75. doi: 10.1179/2047773214Y.0000000130. Epub 2014 Mar 7. Pathog Glob Health. 2014. PMID: 24601908 Free PMC article. Review.
-
Regulatory Functions of Hypoxia in Host-Parasite Interactions: A Focus on Enteric, Tissue, and Blood Protozoa.Microorganisms. 2023 Jun 16;11(6):1598. doi: 10.3390/microorganisms11061598. Microorganisms. 2023. PMID: 37375100 Free PMC article. Review.
References
-
- White NJ, Ho M. The pathophysiology of malaria. Adv. Parasitol. 1992;31:83–173. - PubMed
-
- World Health Organization CDC Severe falciparum malaria. Trans. R. Soc. Trop. Med. Hyg. 2000;94(Suppl. 1):S1–S90. - PubMed
-
- Pongponratn E, Turner GD, Day NP, et al. An ultrastructural study of the brain in fatal Plasmodium falciparum malaria. Am. J. Trop. Med. Hyg. 2003;69:345–359. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
