

Review
doi: 10.1161/CIRCEP.109.921056.
Short QT syndrome: from bench to bedside
Affiliations
- PMID: 20716721
- PMCID: PMC2933105
- DOI: 10.1161/CIRCEP.109.921056
Item in Clipboard
Review
Short QT syndrome: from bench to bedside
Circ Arrhythm Electrophysiol.
2010 Aug.
No abstract available
Figures
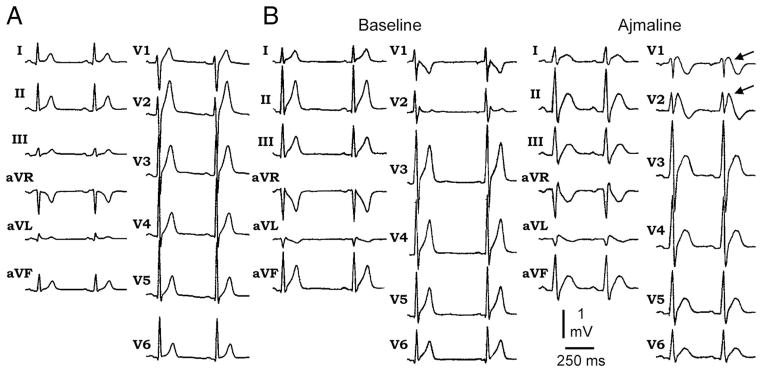
A, Twelve-lead ECG showing characteristic ECG features of SQTS. B, Twelve-lead ECG showing characteristic ECG features of new clinical entity with combined ECG phenotype of Brugada syndrome in addition to SQTS. The ECG shows Brugada-type ST elevation in V1 and V2 after administration of ajmaline in addition to short QT interval. Modified from References and with permission. ,

A, Reduced rate-adaptation of QT interval. The QT-RR relationship is less linear and its slope is less steep in the SQTS patient as compared with control subjects. Quinidine restores the relationship toward control values. QTpV3 denotes the interval from the beginning of QRS complex to peak of T wave, measured in lead V3. Reproduced from Reference , with permission. B, Holter monitoring showing impaired adjustment of QT interval with change in heart rate.

PD-118057 (IKr agonist) model of SQTS in canine left ventricular wedge. A, PD-118057 induced abbreviation of QT interval and increase in TDR. Preferential abbreviation of epicardial action potential results in an increase in TDR. Each panel shows transmembrane action potentials simultaneously recorded from an epicardial (Epi) and a deep subendocardial M cell in an arterially perfused LV wedge preparation, together with a pseudo-ECG. Basic cycle length, 2000 ms. B, Programmed electric stimulation applied to epicardium induced polymorphic VT in the presence of PD-110857 but not after addition of quinidine. Basic cycle length, 2000 ms. Modified with permission.

Self-terminating episode of polymorphic VT in a patient with SQTS: Lead V3. The episode is precipitated by an extrasystole with a very short coupling interval.
Similar articles
-
MY APPROACH to early repolarization syndrome.Trends Cardiovasc Med. 2016 May;26(4):393-4. doi: 10.1016/j.tcm.2015.08.008. Epub 2016 Jan 29. Trends Cardiovasc Med. 2016. PMID: 26944231 No abstract available.
-
Troubleshooting implanted cardioverter defibrillator sensing problems I.Circ Arrhythm Electrophysiol. 2014 Dec;7(6):1237-61. doi: 10.1161/CIRCEP.114.002344. Circ Arrhythm Electrophysiol. 2014. PMID: 25516582 Review. No abstract available.
-
Multiple clinical profiles of families with the short QT syndrome.Europace. 2018 Jun 1;20(FI1):f113-f121. doi: 10.1093/europace/eux186. Europace. 2018. PMID: 29016797
-
The diagnosis, significance, and management of A-V nodal rhythms.Cardiovasc Clin. 1970;2(2):145-62. Cardiovasc Clin. 1970. PMID: 4131123 Review. No abstract available.
-
Implantable Defibrillator Timing Windows: When Coincidence Can Be Confusing.Circ Arrhythm Electrophysiol. 2016 Mar;9(3):e002876. doi: 10.1161/CIRCEP.115.002876. Circ Arrhythm Electrophysiol. 2016. PMID: 26902146 No abstract available.
Cited by
-
Probucol-induced hERG Channel Reduction can be Rescued by Matrine and Oxymatrine in vitro.Curr Pharm Des. 2020;25(43):4606-4612. doi: 10.2174/1381612825666191026170033. Curr Pharm Des. 2020. PMID: 31657676 Free PMC article.
-
Comparison of K+ Channel Families.Handb Exp Pharmacol. 2021;267:1-49. doi: 10.1007/164_2021_460. Handb Exp Pharmacol. 2021. PMID: 34247281
-
Genetic risk factors for drug-induced long QT syndrome: findings from a large real-world case-control study.Pharmacogenomics. 2024 Feb;25(3):117-131. doi: 10.2217/pgs-2023-0229. Epub 2024 Mar 20. Pharmacogenomics. 2024. PMID: 38506312 Free PMC article.
-
Genetics of inherited primary arrhythmia disorders.Appl Clin Genet. 2015 Sep 18;8:215-33. doi: 10.2147/TACG.S55762. eCollection 2015. Appl Clin Genet. 2015. PMID: 26425105 Free PMC article. Review.
-
Overview of Basic Mechanisms of Cardiac Arrhythmia.Card Electrophysiol Clin. 2011 Mar 1;3(1):23-45. doi: 10.1016/j.ccep.2010.10.012. Card Electrophysiol Clin. 2011. PMID: 21892379 Free PMC article. No abstract available.
References
-
- Gussak I, Brugada P, Brugada J, Wright RS, Kopecky SL, Chaitman BR, Bjerregaard P. Idiopathic short QT interval: a new clinical syndrome? Cardiology. 2000;94:99–102. - PubMed
-
- Gussak I, Antzelevitch C, Goodman D, Bjerregaard P. Short QT interval: ECG phenomenon and clinical syndrome. In: Gussak I, Antzelevitch C, editors. Cardiac Repolarization. Bridging Basic and Clinical Sciences. Totowa, NJ: Humana Press; 2003. pp. 497–506.
-
- Gussak I, Bjerregaard P. Short QT syndrome: 5 years of progress. J Electrocardiol. 2005;38:375–377. - PubMed
-
- Giustetto C, Di Monte F, Wolpert C, Borggrefe M, Schimpf R, Sbragia P, Leone G, Maury P, Anttonen O, Haissaguerre M, Gaita F. Short QT syndrome: clinical findings and diagnostic-therapeutic implications. Eur Heart J. 2006;27:2440–2447. - PubMed
-
- Gaita F, Giustetto C, Bianchi F, Wolpert C, Schimpf R, Riccardi R, Grossi S, Richiardi E, Borggrefe M. Short QT syndrome: a familial cause of sudden death. Circulation. 2003;108:965–970. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
