

Dosimetric performance of the new high-definition multileaf collimator for intracranial stereotactic radiosurgery
- PMID: 20717077
- PMCID: PMC5720445
- DOI: 10.1120/jacmp.v11i3.3040
Dosimetric performance of the new high-definition multileaf collimator for intracranial stereotactic radiosurgery
Abstract
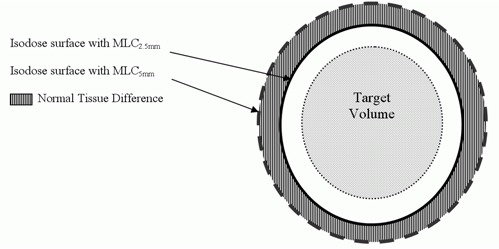
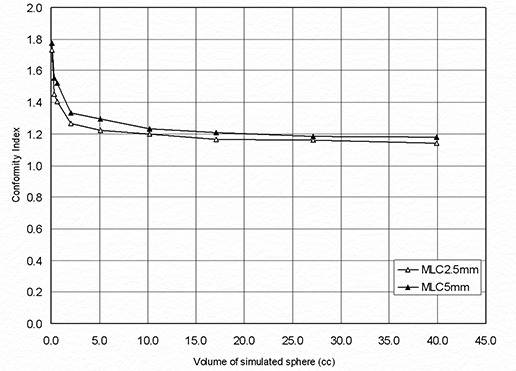
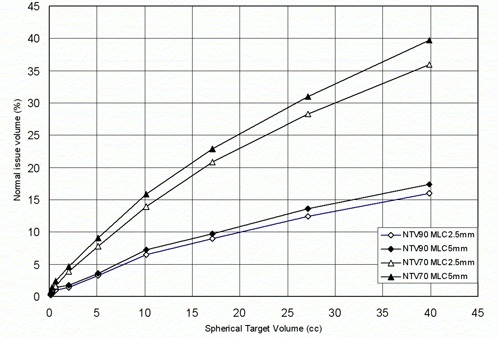
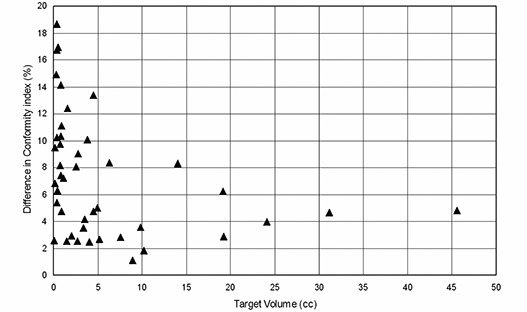
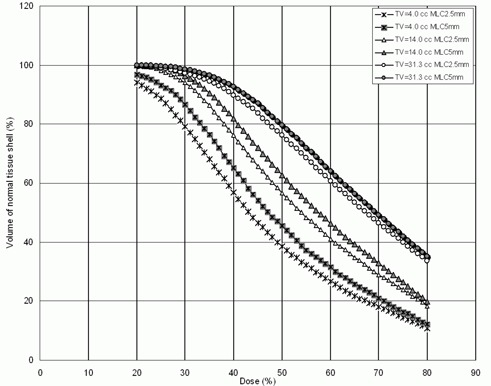
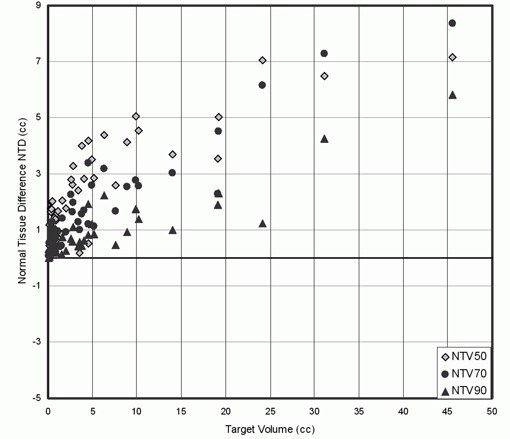
The objective was to evaluate the performance of a high-definition multileaf collimator (MLC) of 2.5 mm leaf width (MLC2.5) and compare to standard 5 mm leaf width MLC (MLC5) for the treatment of intracranial lesions using dynamic conformal arcs (DCA) technique with a dedicated radiosurgery linear accelerator. Simulated cases of spherical targets were created to study solely the effect of target volume size on the performance of the two MLC systems independent of target shape complexity. In addition, 43 patients previously treated for intracranial lesions in our institution were retrospectively planned using DCA technique with MLC2.5 and MLC5 systems. The gross tumor volume ranged from 0.07 to 40.57 cm3 with an average volume of 5.9 cm3. All treatment parameters were kept the same for both MLC-based plans. The plan evaluation was performed using figures of merits (FOM) for a rapid and objective assessment on the quality of the two treatment plans for MLC2.5 and MLC5. The prescription isodose surface was selected as the greatest isodose surface covering >or= 95% of the target volume and delivering 95% of the prescription dose to 99% of target volume. A Conformity Index (CI) and conformity distance index (CDI) were used to quantifying the dose conformity to a target volume. To assess normal tissue sparing, a normal tissue difference (NTD) was defined as the difference between the volume of normal tissue receiving a certain dose utilizing MLC5 and the volume receiving the same dose using MLC2.5. The CI and normal tissue sparing for the simulated spherical targets were better with the MLC2.5 as compared to MLC5. For the clinical patients, the CI and CDI results indicated that the MLC2.5 provides better treatment conformity than MLC5 even at large target volumes. The CI's range was 1.15 to 2.44 with a median of 1.59 for MLC2.5 compared to 1.60-2.85 with a median of 1.71 for MLC5. Improved normal tissue sparing was also observed for MLC2.5 over MLC5, with the NTD always positive, indicating improvement, and ranging from 0.1 to 8.3 for normal tissue receiving 50% (NTV50), 70% (NTV70) and 90% (NTV90) of the prescription dose. The MLC2.5 has a dosimetric advantage over the MLC5 in Linac-based radiosurgery using DCA method for intracranial lesions, both in treatment conformity and normal tissue sparing when target shape complexity increases.
Figures
Similar articles
-
Dosimetric study using different leaf-width MLCs for treatment planning of dynamic conformal arcs and intensity-modulated radiosurgery.Med Phys. 2005 Feb;32(2):405-11. doi: 10.1118/1.1842911. Med Phys. 2005. PMID: 15789586
-
Impact of collimator leaf width and treatment technique on stereotactic radiosurgery and radiotherapy plans for intra- and extracranial lesions.Radiat Oncol. 2009 Jan 21;4:3. doi: 10.1186/1748-717X-4-3. Radiat Oncol. 2009. PMID: 19159471 Free PMC article.
-
Comparison of a micro-multileaf collimator with a 5-mm-leaf-width collimator for intracranial stereotactic radiotherapy.Int J Radiat Oncol Biol Phys. 2003 Dec 1;57(5):1443-9. doi: 10.1016/s0360-3016(03)01579-7. Int J Radiat Oncol Biol Phys. 2003. PMID: 14630284
-
Impact of the high-definition multileaf collimator on linear accelerator-based intracranial stereotactic radiosurgery.Br J Radiol. 2011 Jul;84(1003):629-38. doi: 10.1259/bjr/19726857. Epub 2010 Oct 5. Br J Radiol. 2011. PMID: 20923911 Free PMC article.
-
A mini review of plan quality and secondary cancer risk in CyberKnife M6 radiosurgery for benign intracranial tumors.Front Oncol. 2024 Aug 7;14:1453256. doi: 10.3389/fonc.2024.1453256. eCollection 2024. Front Oncol. 2024. PMID: 39175469 Free PMC article. Review.
Cited by
-
Dosimetric Comparison, Treatment Efficiency Estimation, and Biological Evaluation of Popular Stereotactic Radiosurgery Options in Treating Single Small Brain Metastasis.Front Oncol. 2021 Aug 5;11:716152. doi: 10.3389/fonc.2021.716152. eCollection 2021. Front Oncol. 2021. PMID: 34540686 Free PMC article.
-
Is there a volume threshold of brain metastases for Linac-based stereotactic radiotherapy?J Radiosurg SBRT. 2021;7(4):309-319. J Radiosurg SBRT. 2021. PMID: 34631232 Free PMC article.
-
Dosimetric comparison of different treatment modalities for stereotactic radiotherapy.Radiat Oncol. 2017 Sep 16;12(1):155. doi: 10.1186/s13014-017-0890-0. Radiat Oncol. 2017. PMID: 28915893 Free PMC article.
-
Feasibility of using the Vero SBRT system for intracranial SRS.J Appl Clin Med Phys. 2014 Jan 6;15(1):4437. doi: 10.1120/jacmp.v15i1.4437. J Appl Clin Med Phys. 2014. PMID: 24423838 Free PMC article.
-
Dosimetric Performance and Planning/Delivery Efficiency of a Dual-Layer Stacked and Staggered MLC on Treating Multiple Small Targets: A Planning Study Based on Single-Isocenter Multi-Target Stereotactic Radiosurgery (SRS) to Brain Metastases.Front Oncol. 2019 Jan 22;9:7. doi: 10.3389/fonc.2019.00007. eCollection 2019. Front Oncol. 2019. PMID: 30723702 Free PMC article.
References
-
- Smith V, Verhey L, Serago CF. Comparison of radiosurgery treatment modalities based on complication and control probabilities. Int J Radiat Oncol Biol Phys. 1998;40(2):507–13. - PubMed
-
- Shaw E, Kline R, Gillin M, et al. Radiation Therapy Oncology Group: radiosurgery quality assurance guidelines. Int J Radiat Oncol Biol Phys. 1993;27(5):1231–39. - PubMed
-
- Nedzi LA, Kooy HM, Alexander E, 3rd, Svensson GK, Loeffler JS. Dynamic field shaping for stereotactic radiosurgery: a modeling study. Int J Radiat Oncol Biol Phys. 1993;25(5):859–69. - PubMed
-
- Shaw E, Scott C, Souhami L, et al. Single dose radiosurgical treatment of recurrent previously irradiated primary brain tumors and brain metastases: final report of RTOG protocol 90‐05. Int J Radiat Oncol Biol Phys. 2000;47(2):291–98. - PubMed
-
- Drzymala RE, Mohan R, Brewster L, et al. Dose‐volume histograms. Int J Radiat Oncol Biol Phys. 1991;21(1):71–78. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
