

A comprehensive study on decreasing the kilovoltage cone-beam CT dose by reducing the projection number
- PMID: 20717096
- PMCID: PMC5720437
- DOI: 10.1120/jacmp.v11i3.3274
A comprehensive study on decreasing the kilovoltage cone-beam CT dose by reducing the projection number
Abstract
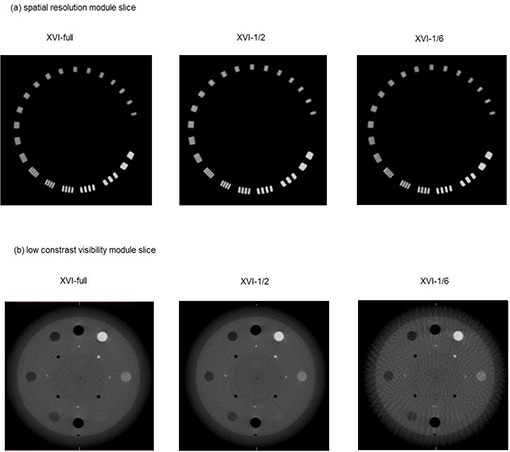
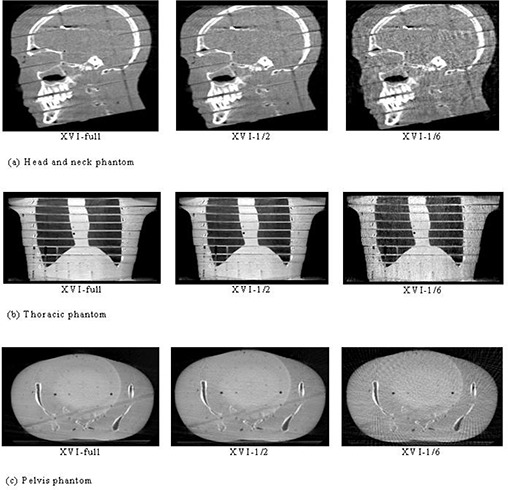
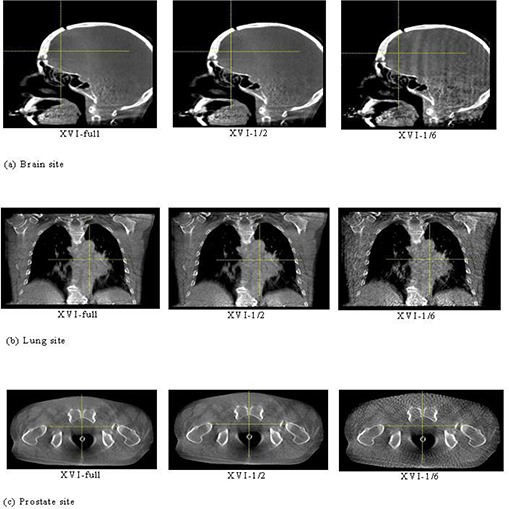
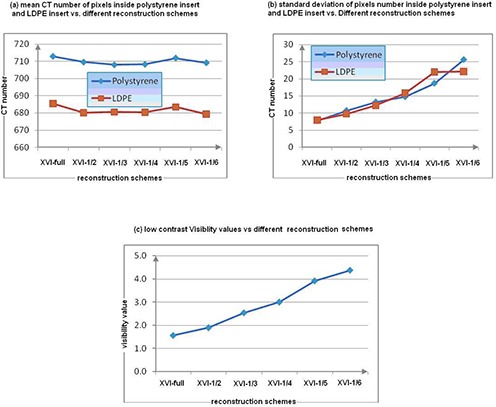
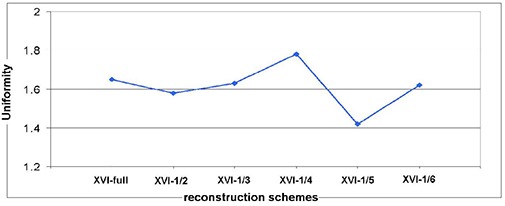
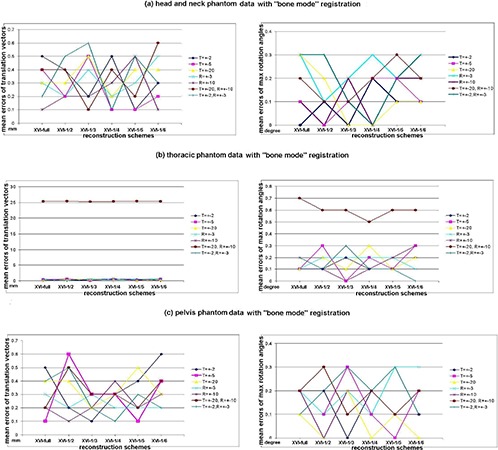
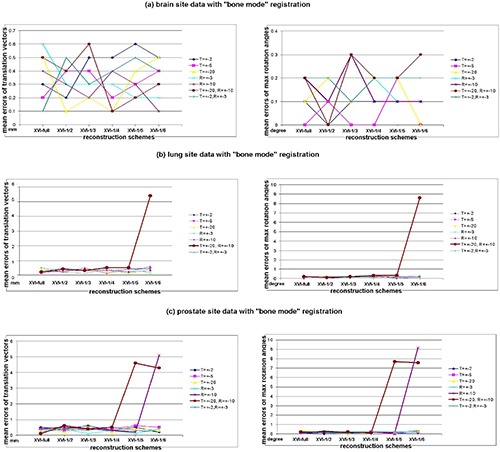
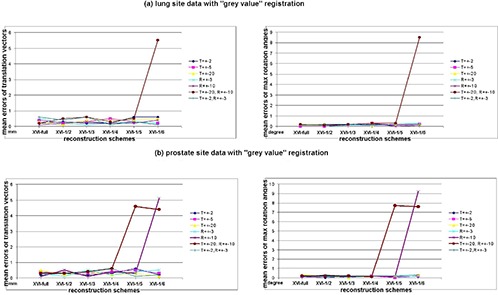
The objective of this study was to evaluate the effect of kilovoltage cone-beam computed tomography (CBCT) on registration accuracy and image qualities with a reduced number of planar projections used in volumetric imaging reconstruction. The ultimate goal is to evaluate the possibility of reducing the patient dose while maintaining registration accuracy under different projection-number schemes for various clinical sites. An Elekta Synergy Linear accelerator with an onboard CBCT system was used in this study. The quality of the Elekta XVI cone-beam three-dimensional volumetric images reconstructed with a decreasing number of projections was quantitatively evaluated by a Catphan phantom. Subsequently, we tested the registration accuracy of imaging data sets on three rigid anthropomorphic phantoms and three real patient sites under the reduced projection-number (as low as 1/6th) reconstruction of CBCT data with different rectilinear shifts and rota-tions. CBCT scan results of the Catphan phantom indicated the CBCT images got noisier when the number of projections was reduced, but their spatial resolution and uniformity were hardly affected. The maximum registration errors under the small amount transformation of the reference CT images were found to be within 0.7 mm translation and 0.3 masculine rotation. However, when the projection number was lower than one-fourth of the full set with a large amount of transformation of reference CT images, the registration could easily be trapped into local minima solutions for a nonrigid anatomy. We concluded, by using projection-number reduction strategy under conscientious care, imaging-guided localization procedure could achieve a lower patient dose without losing the registration accuracy for various clinical sites and situations. A faster scanning time is the main advantage compared to the mA decrease-based, dose-reduction method.
Figures
References
-
- Chauvet B, de Rauglaudre G, Mineur L, Alfonsi M. Reboul F. [Dose‐response relationship in radiotherapy: an evidence?]. Cancer Radiother. 2003;7 Suppl 1:8s–14s. - PubMed
-
- Islam MK, Purdie TG, Norrlinger BD, et al. Patient dose from kilovoltage cone beam computed tomography imaging in radiation therapy. Med Phys. 2006;33(6):1573–82. - PubMed
-
- Pisani L, Lockman D, Jaffray D, Yan D, Martinez A, Wong, J . Setup error in radiotherapy: on‐line correction using electronic kilovoltage and megavoltage radiographs. Int J Radiat Oncol Biol Phys. 2000;47(3):825–39. - PubMed
-
- Jaffray DA, Drake DG, Moreau M, Martinez AA, Wong, JW . A radiographic and tomographic imaging system integrated into a medical linear accelerator for localization of bone and soft‐tissue targets. Int J Radiat Oncol Biol Phys. 1999;45(3):773–89. - PubMed
-
- Jaffray DA, Siewerdsen JH. Cone‐beam computed tomography with a flat‐panel imager: initial performance characterization. Med Phys. 2000;27(6):1311–23. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
