

The cytokine response to human traumatic brain injury: temporal profiles and evidence for cerebral parenchymal production
- PMID: 20717122
- PMCID: PMC3049520
- DOI: 10.1038/jcbfm.2010.142
The cytokine response to human traumatic brain injury: temporal profiles and evidence for cerebral parenchymal production
Abstract
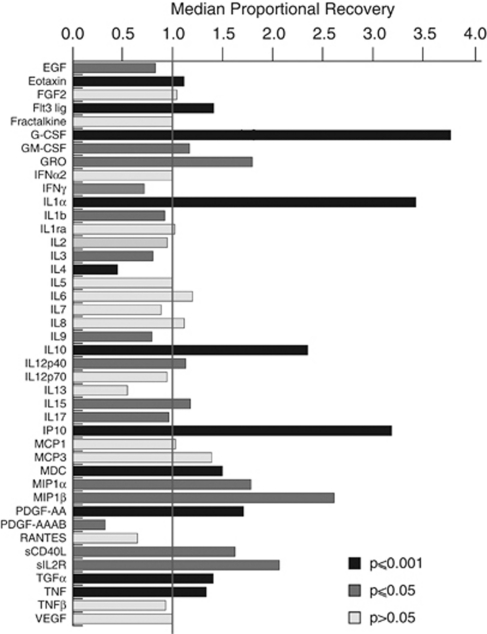
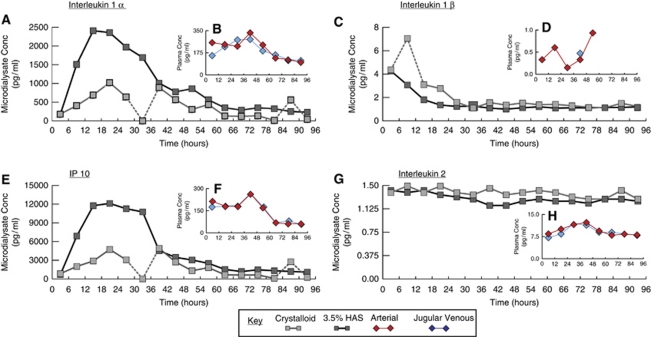
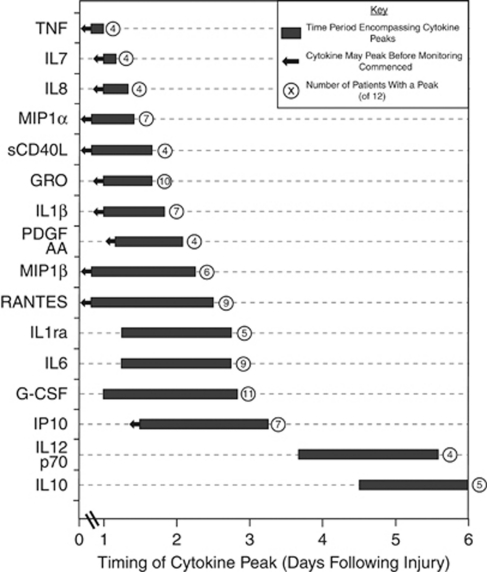
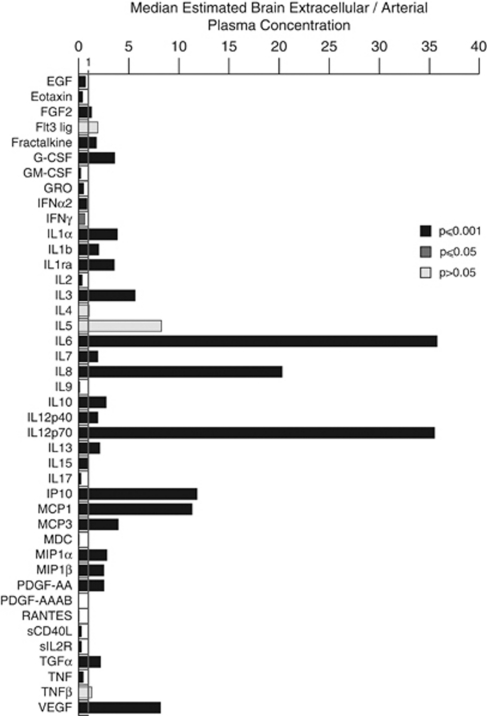
The role of neuroinflammation is increasingly being recognised in a diverse range of cerebral pathologies, including traumatic brain injury (TBI). We used cerebral microdialysis and paired arterial and jugular bulb plasma sampling to characterise the production of 42 cytokines after severe TBI in 12 patients over 5 days. We compared two microdialysis perfusates in six patients: central nervous system perfusion fluid and 3.5% human albumin solution (HAS); 3.5% HAS has a superior fluid recovery (95.8 versus 83.3%), a superior relative recovery in 18 of 42 cytokines (versus 8 of 42), and a qualitatively superior recovery profile. All 42 cytokines were recovered from the human brain. Sixteen cytokines showed a stereotyped temporal peak, at least twice the median value for that cytokine over the monitoring period; day 1: tumour necrosis factor, interleukin (IL)7, IL8, macrophage inflammatory protein (MIP)1α, soluble CD40 ligand, GRO, IL1β, platelet derived growth factor (PDGF)-AA, MIP1β, RANTES; day 2: IL1 receptor antagonist (ra). IL6, granulocyte-colony stimulating factor (G-CSF), chemokine CXC motif ligand 10 (IP10); days 4 to 5: IL12p70, IL10. Brain extracellular fluid concentrations were significantly higher than plasma concentrations for 19 cytokines: basic fibroblast growth factor (FGF2), G-CSF, IL1α, IL1β, IL1ra, IL3, IL6, IL8, IL10, IL12p40, IL12p70, IP10, monocyte chemotactic protein (MCP)1, MCP3, MIP1α, MIP1β, PDGF-AA, transforming growth factor (TGF)α and vascular endothelial growth factor. No clear arterio-jugular venous gradients were apparent. These data provide evidence for the cerebral production of these cytokines and show a stereotyped temporal pattern after TBI.
Figures
References
-
- Banks WA, Erickson MA. The blood-brain barrier and immune function and dysfunction. Neurobiol Dis. 2010;37:26–32. - PubMed
-
- Bellander BM, Cantais E, Enblad P, Hutchinson P, Nordstrom CH, Robertson C, Sahuquillo J, Smith M, Stocchetti N, Ungerstedt U, Unterberg A, Olsen NV. Consensus meeting on microdialysis in neurointensive care. Intensive Care Med. 2004;30:2166–2169. - PubMed
-
- Berger RP, Táasan S, Rand A, Lokshin A, Kochanek P. Multiplex assessment of serum biomarker concentrations in well-appearing children with inflicted traumatic brain injury. Pediatr Res. 2009;65:97–102. - PubMed
-
- Buttram SD, Wisniewski SR, Jackson EK, Adelson PD, Feldman K, Bayir H, Berger RP, Clark RS, Kochanek PM. Multiplex assessment of cytokine and chemokine levels in cerebrospinal fluid following severe pediatric traumatic brain injury: effects of moderate hypothermia. J Neurotrauma. 2007;24:1707–1717. - PubMed
-
- Chiaretti A, Antonelli A, Mastrangelo A, Pezzotti P, Tortorolo L, Tosi F, Genovese O. Interleukin-6 and nerve growth factor upregulation correlates with improved outcome in children with severe traumatic brain injury. J Neurotrauma. 2008;25:225–234. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
