

The Frank Stinchfield Award: the impact of socioeconomic factors on outcome after THA: a prospective, randomized study
- PMID: 20717856
- PMCID: PMC3018201
- DOI: 10.1007/s11999-010-1519-x
The Frank Stinchfield Award: the impact of socioeconomic factors on outcome after THA: a prospective, randomized study
Abstract
Background: Most studies of total hip arthroplasty (THA) focus on the effect of the type of implant on the clinical result. Relatively little data are available on the impact of the patient's preoperative status and socioeconomic factors on the clinical results following THA.
Questions/purposes: We determined the relative importance of patient preoperative and socioeconomic status compared to implant and technique factors in predicting patient outcome as reflected by scores on commonly utilized rating scales (eg, Harris Hip Score, WOMAC, SF-12, degree of patient satisfaction, or presence or severity of thigh pain) following cementless THA.
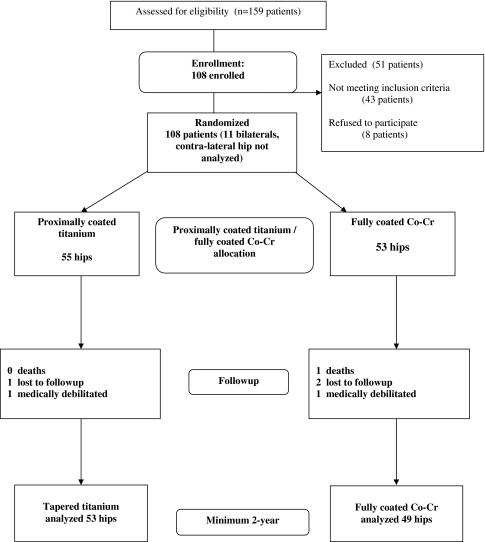
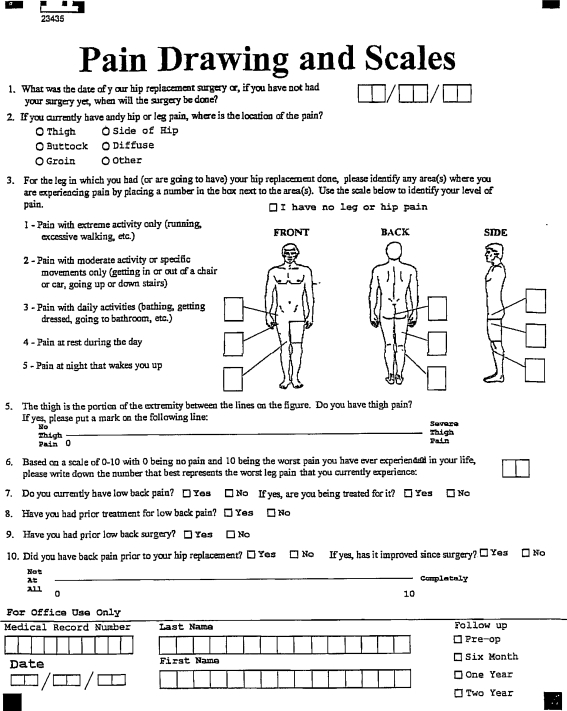
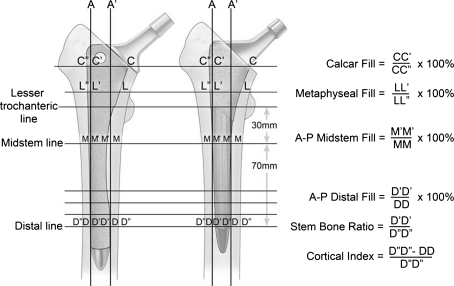
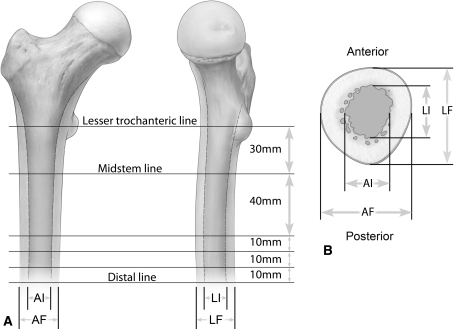
Methods: All patients during the study period were offered enrollment in a prospective, randomized study to receive either a titanium, tapered, proximally coated stem; or a Co-Cr, cylindrical, extensively coated stem; 102 patients were enrolled. We collected detailed patient data preoperatively including diagnosis, age, gender, insurance status, medical comorbidities, tobacco and alcohol use, household income, educational level, and history of treatment for lumbar spine pathology. Clinical evaluation included Harris Hip Score, SF-12, WOMAC, pain drawing, and UCLA activity rating and satisfaction questionnaire. Implant factors included stem type, stem size, fit in the canal, and stem-bone stiffness ratios. Minimum 2 year followup was obtained in 95% of the enrolled patients (102 patients).
Results: Patient demographics and preoperative status were more important than implant factors in predicting the presence of thigh pain, dissatisfaction, and a low hip score. The most predictive factors were ethnicity, educational level, poverty level, income, and a low preoperative WOMAC score or preoperative SF-12 mental component score. No implant parameter correlated with outcome or satisfaction.
Conclusion: Socioeconomic factors and preoperative status have more impact on the clinical outcome of cementless THA than implant related factors.
Level of evidence: Level I, prospective, randomized clinical trial. See the guidelines online for a complete description of level of evidence.
Figures
References
-
- Amstutz HC, Thomas BJ, Jinnah R, Kim W, Grogan T, Yale C. Treatment of primary osteoarthritis of the hip. A comparison of total joint and surface replacement arthroplasty. J Bone Joint Surg Am. 1984;66:228–241. - PubMed
-
- Barrack RL, Mulroy RD, Jr, Harris WH. Improved cementing techniques and femoral component loosening in young patients with hip arthroplasty. A 12-year radiographic review. J Bone Joint Surg Br. 1992;74:385–389. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
