

The John Charnley Award: risk factors for cup malpositioning: quality improvement through a joint registry at a tertiary hospital
- PMID: 20717858
- PMCID: PMC3018230
- DOI: 10.1007/s11999-010-1487-1
The John Charnley Award: risk factors for cup malpositioning: quality improvement through a joint registry at a tertiary hospital
Abstract
Background: Few studies have examined factors that affect acetabular cup positioning. Since cup positioning has been linked to dislocation and increased bearing surface wear, these factors affecting cup position are important considerations.
Question/purposes: We determined the percent of optimally positioned acetabular cups and whether patient and surgical factors affected acetabular component position.
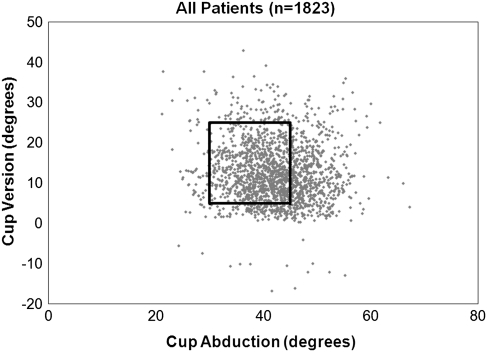
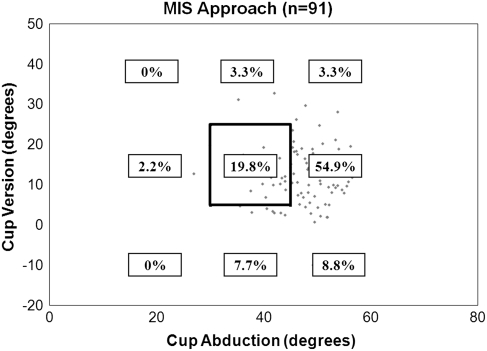
Methods: We obtained postoperative AP pelvis and cross-table lateral radiographs on 2061 consecutive patients who received a THA or hip resurfacing from 2004 to 2008. One thousand nine hundred and fifty-two hips had AP pelvic radiographs with correct position of the hip center, and 1823 had both version and abduction angles measured. The AP radiograph was measured using Hip Analysis Suite™ to calculate the cup inclination and version angles, using the lateral film to determine version direction. Acceptable ranges were defined for abduction (30°-45°) and version (5°-25°).
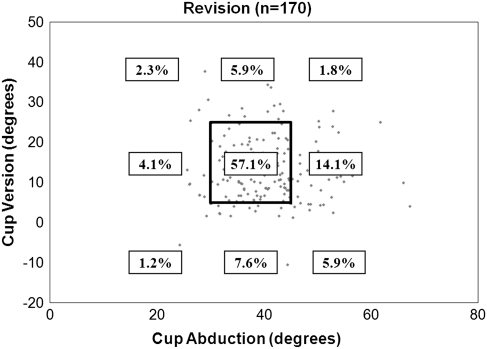
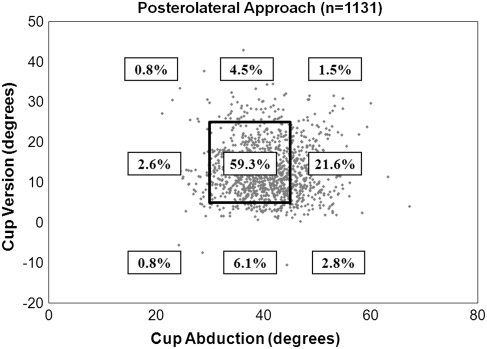
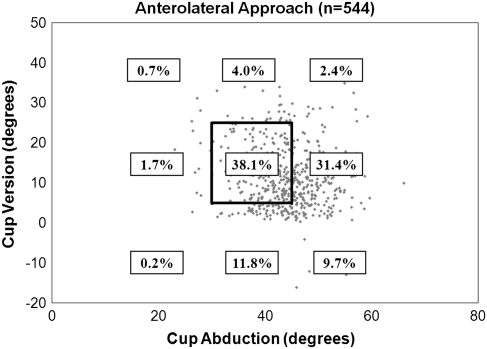
Results: From the 1823 hips, 1144 (63%) acetabular cups were within the abduction range, 1441 (79%) were within the version range, and 917 (50%) were within the range for both. Surgical approach, surgeon volume, and obesity (body mass index > 30) independently predicted malpositioned cups. Comparison of low versus high volume surgeons, minimally invasive surgical versus posterolateral approach, and obesity versus all other body mass index groups showed a twofold (1.5-2.8), sixfold (3.5-10.7), and 1.3-fold (1.1-1.7) increased risk for malpositioned cups, respectively.
Conclusions: Factors correlated to malpositioned cups included surgical approach, surgeon volume, and body mass index with increased risk of malpositioning for minimally invasive surgical approach, low volume surgeons, and obese patients. Further analyses on patient and surgical factors' influence on cup position at a lower volume medical center would provide a valuable comparison.
Level of evidence: Level II, prognostic study. See Guidelines for Authors for a complete description of levels of evidence.
Figures
Comment in
-
[Arthroplasty].Orthopade. 2013 Jan;42(1):55-6. doi: 10.1007/s00132-012-2055-z. Orthopade. 2013. PMID: 23325333 German. No abstract available.
References
-
- Ali Khan MA, Brakenbury PH. IS R Dislocation following total hip replacement. J Bone Joint Surg Br. 1981;63:214–218. - PubMed
-
- Arthursson AJ, Furnes O, Espehaug B, Havelin LI, Soreide JA. Prosthesis survival after total hip arthroplasty—does surgical approach matter? Analysis of 19,304 Charnley and 6,002 Exeter primary total hip arthroplasties reported to the Norwegian Arthroplasty Register. Acta Orthop. 2007;78:719–729. doi: 10.1080/17453670710014482. - DOI - PubMed
-
- Bartz RL, Noble PC, Kadakia NR, Tullos HS. The effect of femoral component head size on posterior dislocation of the artificial hip joint. J Bone Joint Surg Am. 2000;82:1300–1307. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
