

Oxygen distribution in the human eye: relevance to the etiology of open-angle glaucoma after vitrectomy
- PMID: 20720218
- PMCID: PMC3061509
- DOI: 10.1167/iovs.10-5666
Oxygen distribution in the human eye: relevance to the etiology of open-angle glaucoma after vitrectomy
Abstract
Purpose: Vitrectomy, when followed by cataract surgery, increases the risk of open-angle glaucoma. This study was conducted in patients to determine whether these procedures are associated with increased exposure of the trabecular meshwork to oxygen.
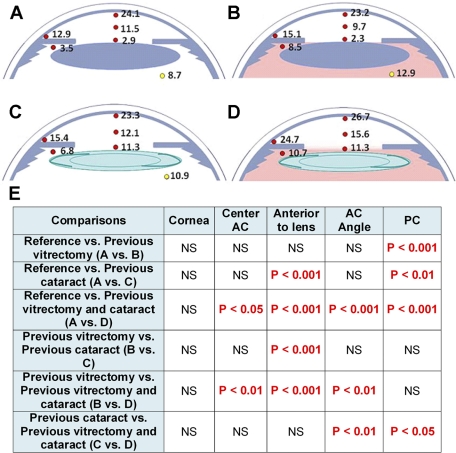
Methods: Oxygen distribution was recorded with a fiberoptic probe in patients undergoing surgery for cataract, glaucoma, or retinal disease. pO(2) was measured beneath the central cornea, in the mid-anterior chamber, and in the anterior chamber angle. In patients who were pseudophakic or were scheduled for cataract extraction, pO(2) was also measured in the posterior chamber and near the lens.
Results: Eyes with no previous cataract or vitrectomy surgery had steep oxygen gradients in the aqueous humor between the cornea and lens. pO(2) was low in the posterior chamber and near the lens. Previous vitrectomy was associated with significantly increased pO(2) in the posterior chamber. Eyes with previous cataract surgery had significantly elevated pO(2) only in the posterior chamber and in front of the intraocular lens (IOL). Eyes that had both vitrectomy and previous cataract surgery had increased pO(2) in the posterior chamber, anterior to the IOL, and in the anterior chamber angle. pO(2) in the posterior chamber and the anterior chamber angle correlated strongly.
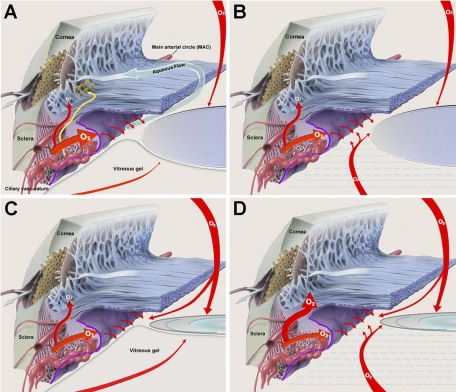
Conclusions: Oxygen metabolism by the lens and cornea establishes oxygen gradients in the anterior segment. Vitrectomy and cataract surgery increase pO(2) in the anterior chamber angle, potentially damaging trabecular meshwork cells. We propose that oxygen levels in the anterior chamber angle are strongly influenced by oxygen derived from the ciliary body circulation.
Figures
References
-
- Gabelt BAT, Kaufman PL. Changes in aqueous humor dynamics with age and glaucoma. Prog Retin Eye Res. 2005;24:612–637 - PubMed
-
- Izzotti A, Bagnis A, Sacca SC. The role of oxidative stress in glaucoma. Mutat Res. 2006;612:105–114 - PubMed
-
- Izzotti A, Sacca SC, Cartiglia C, De Flora S. Oxidative deoxyribonucleic acid damage in the eyes of glaucoma patients. Am J Med. 2003;114:638–646 - PubMed
-
- Izzotti A, Sacca SC, Longobardi M, Cartiglia C. Sensitivity of ocular anterior-chamber tissues to oxidative damage and its relevance to glaucoma pathogenesis. Invest Ophthalmol Vis Sci. 2009;50:5251–5258 - PubMed
-
- Kumar DM, Agarwal N. Oxidative stress in glaucoma: a burden of evidence. J Glaucoma. 2007;16:334–343 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
