

Application of mobile-technology for disease and treatment monitoring of malaria in the "Better Border Healthcare Programme"
- PMID: 20723223
- PMCID: PMC2936405
- DOI: 10.1186/1475-2875-9-237
Application of mobile-technology for disease and treatment monitoring of malaria in the "Better Border Healthcare Programme"
Abstract
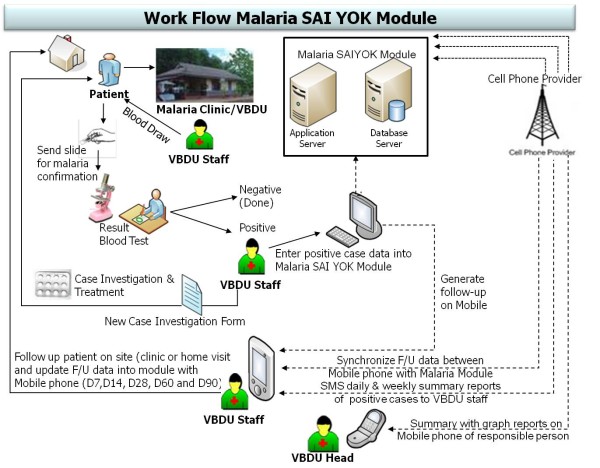
Background: The main objective of this study was to assess the effectiveness of integrating the use of cell-phones into a routine malaria prevention and control programme, to improve the management of malaria cases among an under-served population in a border area. The module for disease and treatment monitoring of malaria (DTMM) consisted of case investigation and case follow-up for treatment compliance and patients' symptoms.
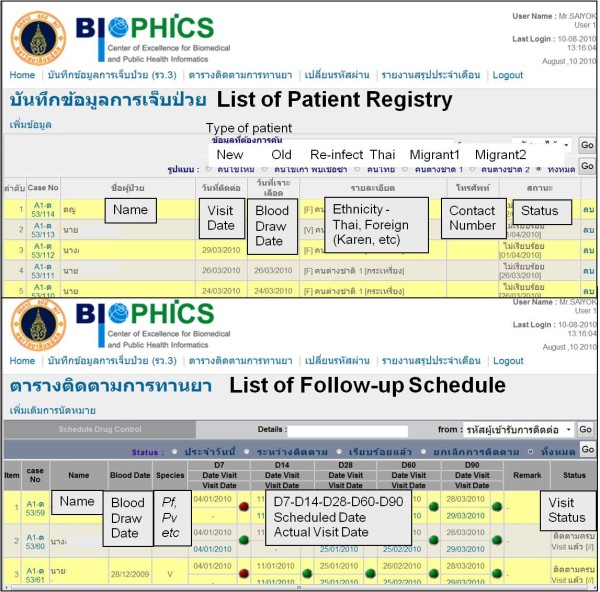
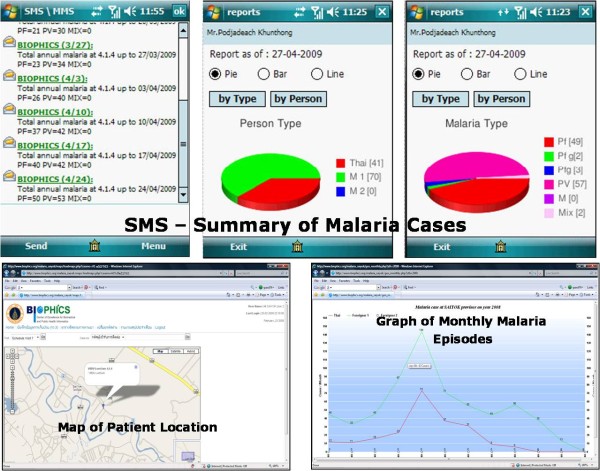
Methods: The module combining web-based and mobile technologies was developed as a proof of concept, in an attempt to replace the existing manual, paper-based activities that malaria staff used in treating and caring for malaria patients in the villages for which they were responsible. After a patient was detected and registered onto the system, case-investigation and treatment details were recorded into the malaria database. A follow-up schedule was generated, and the patient's status was updated when the malaria staff conducted their routine home visits, using mobile phones loaded with the follow-up application module. The module also generated text and graph messages for a summary of malaria cases and basic statistics, and automatically fed to predetermined malaria personnel for situation analysis. Following standard public-health practices, access to the patient database was strictly limited to authorized personnel in charge of patient case management.
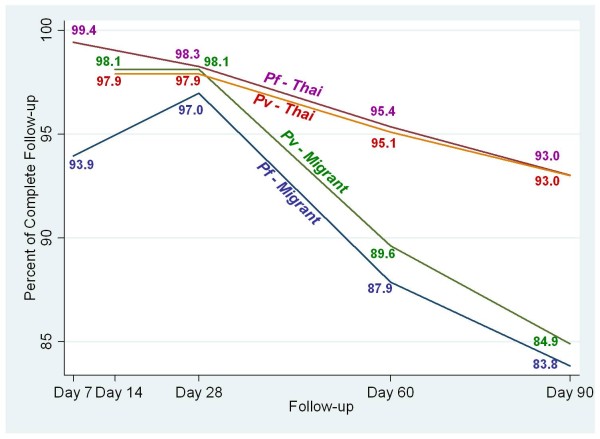
Results: The DTMM module was developed and implemented at the trial site in late November 2008, and was fully functioning in 2009. The system captured 534 malaria patients in 2009. Compared to paper-based data in 2004-2008, the mobile-phone-based case follow-up rates by malaria staff improved significantly. The follow-up rates for both Thai and migrant patients were about 94-99% on Day 7 (Plasmodium falciparum) and Day 14 (Plasmodium vivax) and maintained at 84-93% on Day 90. Adherence to anti-malarial drug therapy, based on self-reporting, showed high completion rate for P. falciparum-infected cases, but lower rate for P. vivax cases. Patients' symptoms were captured onto the mobile phone during each follow-up visit, either during the home visit or at Malaria Clinic; most patients had headache, muscle pain, and fatigue, and some had fever within the first follow-up day (day 7/14) after the first anti-malarial drug dose.
Conclusions: The module was successfully integrated and functioned as part of the malaria prevention and control programme. Despite the bias inherent in sensitizing malaria workers to perform active case follow-up using the mobile device, the study proved for its feasibility and the extent to which community healthcare personnel in the low resource settings could potentially utilize it efficiently to perform routine duties, even in remote areas. The DTMM has been modified and is currently functioning in seven provinces in a project supported by the WHO and the Bill & Melinda Gates Foundation, to contain multi-drug resistant malaria on the Thai-Cambodian border.
Figures

Similar articles
-
Artemisinin resistance containment project in Thailand. (I): Implementation of electronic-based malaria information system for early case detection and individual case management in provinces along the Thai-Cambodian border.Malar J. 2012 Jul 29;11:247. doi: 10.1186/1475-2875-11-247. Malar J. 2012. PMID: 22839508 Free PMC article.
-
Deployment and use of mobile phone technology for real-time reporting of fever cases and malaria treatment failure in areas of declining malaria transmission in Muheza district north-eastern Tanzania.Malar J. 2017 Aug 1;16(1):308. doi: 10.1186/s12936-017-1956-z. Malar J. 2017. PMID: 28764792 Free PMC article.
-
Eliminating Plasmodium falciparum malaria: results from tailoring active case detection approaches to remote populations in forested border areas in north-eastern Cambodia.Malar J. 2021 Feb 22;20(1):108. doi: 10.1186/s12936-021-03622-4. Malar J. 2021. PMID: 33618718 Free PMC article.
-
Designing and deploying caller tunes on mobile phones to promote malaria vaccine uptake in Africa: can the technology acceptance model (TAM) help?Malar J. 2024 Nov 2;23(1):325. doi: 10.1186/s12936-024-05134-3. Malar J. 2024. PMID: 39488704 Free PMC article. Review.
-
New model of tele-healthcare for consultation, diagnosis, and treatment of a cicatricial pemphigoid case using mobile phones for communication among the patient, the clinic dentist, and the oral pathology specialist.J Dent Sci. 2024 Oct;19(4):2381-2384. doi: 10.1016/j.jds.2024.08.010. Epub 2024 Aug 23. J Dent Sci. 2024. PMID: 39347079 Free PMC article. Review. No abstract available.
Cited by
-
mHealth Interventions in Low and Middle-Income Countries: A Systematic Review.Glob J Health Sci. 2016 Sep 1;8(9):54429. doi: 10.5539/gjhs.v8n9p183. Glob J Health Sci. 2016. PMID: 27157176 Free PMC article.
-
Adapting and Evaluating a Brief Advice Tobacco Cessation Intervention in High-reach, Low-resource Settings in India: Protocol for a Cluster Randomized Controlled Trial.JMIR Res Protoc. 2024 Sep 3;13:e57236. doi: 10.2196/57236. JMIR Res Protoc. 2024. PMID: 39225384 Free PMC article.
-
Cost analysis of implementing mHealth intervention for maternal, newborn & child health care through community health workers: assessment of ReMIND program in Uttar Pradesh, India.BMC Pregnancy Childbirth. 2018 Oct 3;18(1):390. doi: 10.1186/s12884-018-2019-3. BMC Pregnancy Childbirth. 2018. PMID: 30285669 Free PMC article.
-
A mobile phone application for malaria case-based reporting to advance malaria surveillance in Myanmar: a mixed methods evaluation.Malar J. 2021 Mar 26;20(1):167. doi: 10.1186/s12936-021-03701-6. Malar J. 2021. PMID: 33771144 Free PMC article.
-
Cell phone-based system (Chaak) for surveillance of immatures of dengue virus mosquito vectors.J Med Entomol. 2013 Jul;50(4):879-89. doi: 10.1603/me13008. J Med Entomol. 2013. PMID: 23926788 Free PMC article.
References
-
- World Health Organization. Malaria elimination: A field manual for low and moderate endemic countries. Geneva: WHO; 2008. ISBN 978 92 4 159608 4.
-
- World Health Organization. Global malaria control and elimination: report of a technical review. Geneva: WHO; 2008. ISBN 978 92 4 159675 6.
-
- World Health Organization. Regional action plan for malaria control and elimination in the western pacific (2010-2015) Geneva: WHO; 2009.
-
- Lines J, Whitty CJM, Hanson K. Prospects for eradication and elimination of malaria: A technical briefing for DFID, December 2007. British Government's Department for International Development (DFID) 2007.
-
- World Health Organization. Report of an Informal Consultation. Phnom Penh; 2007. Containment of malaria multi-drug resistance on the Cambodia-Thailand border.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
