

Predictors and assessment of cognitive dysfunction resulting from ischaemic stroke
- PMID: 20723846
- PMCID: PMC3592203
- DOI: 10.1016/S1474-4422(10)70164-2
Predictors and assessment of cognitive dysfunction resulting from ischaemic stroke
Abstract
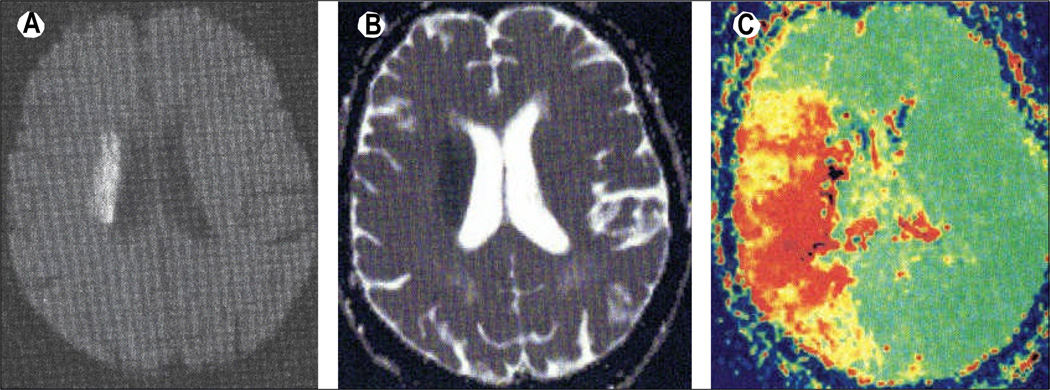
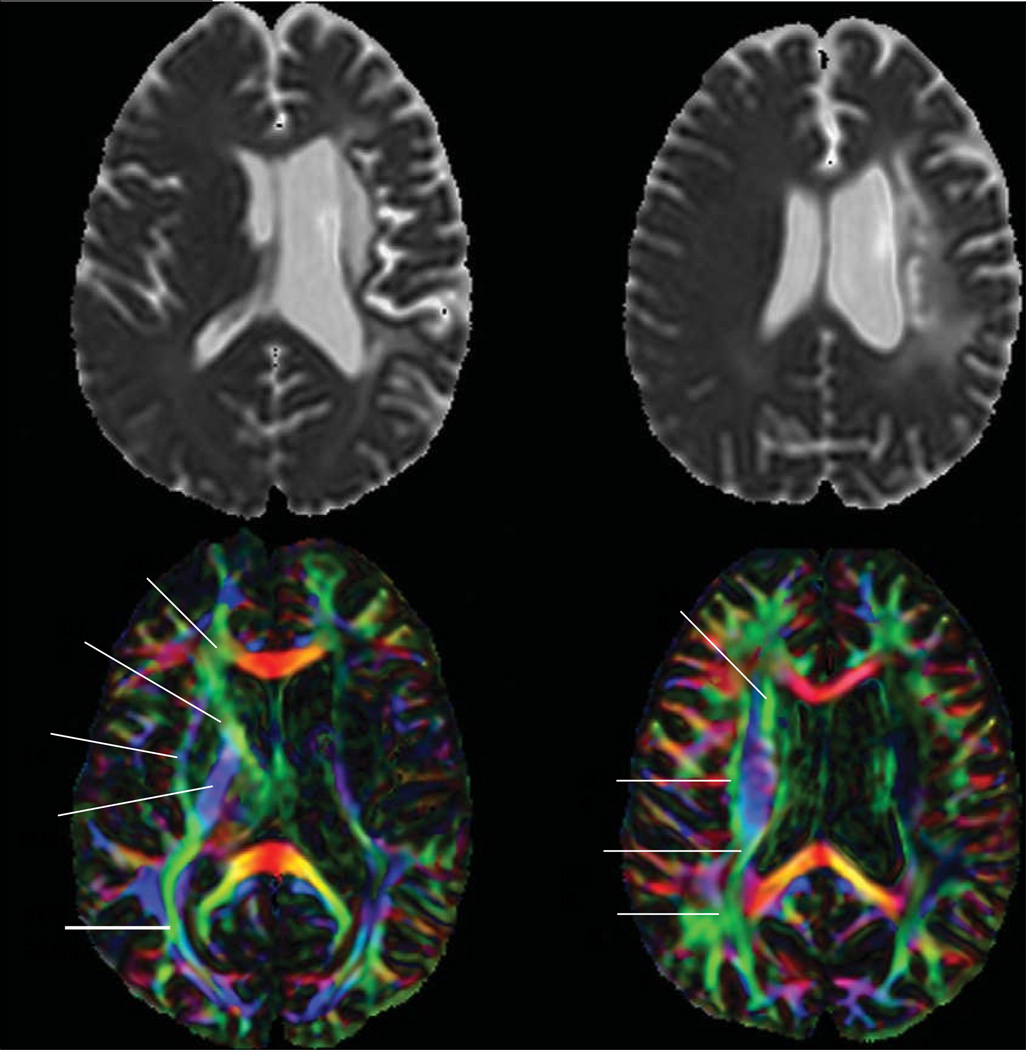
Stroke remains a primary cause of morbidity throughout the world mainly because of its effect on cognition. Individuals can recover from physical disability resulting from stroke, but might be unable to return to their previous occupations or independent life because of cognitive impairments. Cognitive dysfunction ranges from focal deficits, resulting directly from an area of infarction or from hypoperfusion in adjacent tissue, to more global cognitive dysfunction. Global dysfunction is likely to be related to other underlying subclinical cerebrovascular disease, such as white-matter disease or subclinical infarcts. Study of cognitive dysfunction after stroke is complicated by varying definitions and lack of measurement of cognition before stroke. Additionally, stroke can affect white-matter connectivity, so newer imaging techniques, such as diffusion-tensor imaging and magnetisation transfer imaging, that can be used to assess this subclinical injury are important tools in the assessment of cognitive dysfunction after stroke. As research is increasingly focused on the role of preventable risk factors in the development of dementia, the role of stroke in the development of cognitive impairment and dementia could be another target for prevention.
Copyright 2010 Elsevier Ltd. All rights reserved.
Conflict of interest statement
We have no conflicts of interest.
Figures
References
-
- Inatomi Y, Yonehara T, Omiya S, Hashimoto Y, Hirano T, Uchino M. Aphasia during the acute phase in ischemic stroke. Cerebrovasc Dis. 2008;25:316–323. - PubMed
-
- Engelter ST, Gostynski M, Papa S, et al. Epidemiology of aphasia attributable to first ischemic stroke: incidence, severity, fluency, etiology, and thrombolysis. Stroke. 2006;37:1379–1384. - PubMed
-
- Ringman JM, Saver JL, Woolson RF, Clarke WR, Adams HP. Frequency, risk factors, anatomy, and course of unilateral neglect in an acute stroke cohort. Neurology. 2004;63:468–474. - PubMed
-
- Hillis AE, Wityk RJ, Barker PB, et al. Subcortical aphasia and neglect in acute stroke: the role of cortical hypoperfusion. Brain. 2002;125:1094–1104. - PubMed
-
- Hillis AE, Wityk RJ, Tuffiash E, et al. Hypoperfusion of Wernicke’s area predicts severity of semantic deficit in acute stroke. Ann Neurol. 2001;50:561–566. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
