

Prostate secretions from men with chronic pelvic pain syndrome inhibit proinflammatory mediators
- PMID: 20723928
- PMCID: PMC3660015
- DOI: 10.1016/j.juro.2010.05.086
Prostate secretions from men with chronic pelvic pain syndrome inhibit proinflammatory mediators
Abstract
Purpose: In the past numerous chemokines have been noted in the expressed prostatic secretions of patients with chronic prostatitis/chronic pelvic pain syndrome. We examined the functional effects of chemokines in expressed prostatic secretions of patients with chronic pelvic pain syndrome.
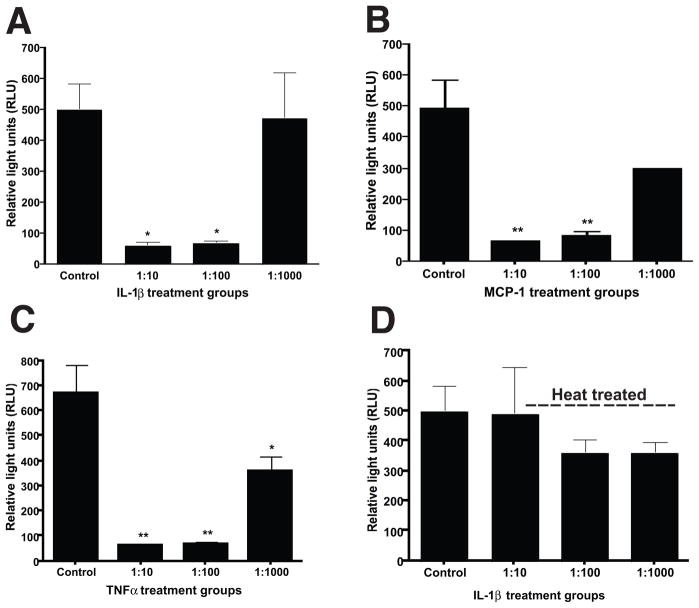
Materials and methods: We studied the functional effects of expressed prostatic secretions on human monocytes by examining monocyte chemotaxis in response to monocyte chemoattractant protein-1, a major chemoattractant previously identified in chronic prostatitis/chronic pelvic pain syndrome cases. We determined effects on cellular signaling by quantifying intracellular calcium increase in monocytes and nuclear factor-κB activation in normal prostate epithelial cells.
Results: Results show that the monocyte chemoattractant protein-1 in expressed prostatic secretions is nonfunctional with an inability to mediate human monocyte chemotaxis, or mediate signaling in monocytes or prostate epithelial cells. This lack of functionality could be extended to other proinflammatory cytokines, such as interleukin-1β and tumor necrosis factor-α, when incubated with expressed prostatic secretions from patients with chronic pelvic pain syndrome. The mechanism underlying this apparent ability to modulate proinflammatory cytokines involves heat labile extracellular proteases that mediate the inhibition of immune and prostate epithelial cell function.
Conclusions: These results may have implications for the design of specific diagnostic and therapeutic methods targeted toward the complete resolution of prostate inflammatory insults.
Copyright © 2010 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures



Comment in
-
Chronic pelvic pain syndrome: a role for aberrant cytokine function.J Urol. 2010 Oct;184(4):1253-4. doi: 10.1016/j.juro.2010.07.007. Epub 2010 Aug 17. J Urol. 2010. PMID: 20723919 No abstract available.
References
-
- Collins MM, Stafford RS, O’Leary MP, et al. How common is prostatitis? A national survey of physician visits. J Urol. 1998;159:1224. - PubMed
-
- Nickel JC, Alexander RB, Schaeffer AJ, et al. Leukocytes and bacteria in men with chronic prostatitis/chronic pelvic pain syndrome compared to asymptomatic controls. J Urol. 2003;170:818. - PubMed
-
- Schaeffer AJ, Knauss JS, Landis JR, et al. Leukocyte and bacterial counts do not correlate with severity of symptoms in men with chronic prostatitis: the National Institutes of Health Chronic Prostatitis Cohort Study. J Urol. 2002;168:1048. - PubMed
-
- True LD, Berger RE, Rothman I, et al. Prostate histopathology and the chronic prostatitis/chronic pelvic pain syndrome: a prospective biopsy study. J Urol. 1999;162:2014. - PubMed
-
- Nickel JC, Roehrborn CG, O’Leary MP, et al. Examination of the relationship between symptoms of prostatitis and histological inflammation: baseline data from the REDUCE chemoprevention trial. J Urol. 2007;178:896. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
