

PrPC, the cellular isoform of the human prion protein, is a novel biomarker of HIV-associated neurocognitive impairment and mediates neuroinflammation
- PMID: 20724601
- PMCID: PMC2947280
- DOI: 10.2353/ajpath.2010.091006
PrPC, the cellular isoform of the human prion protein, is a novel biomarker of HIV-associated neurocognitive impairment and mediates neuroinflammation
Abstract
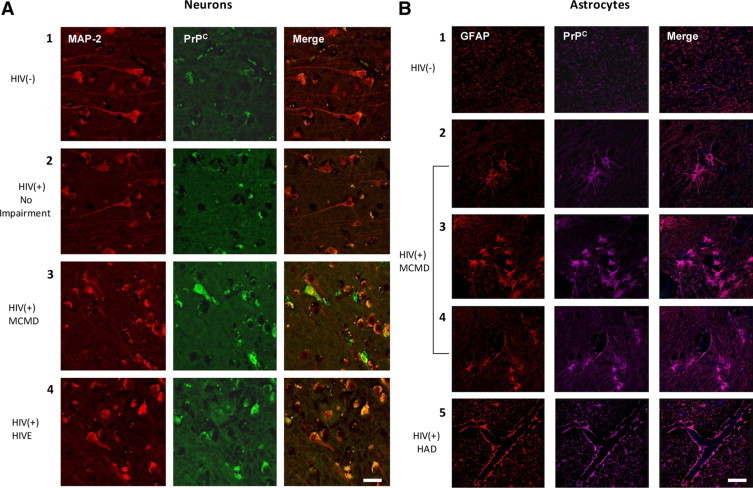
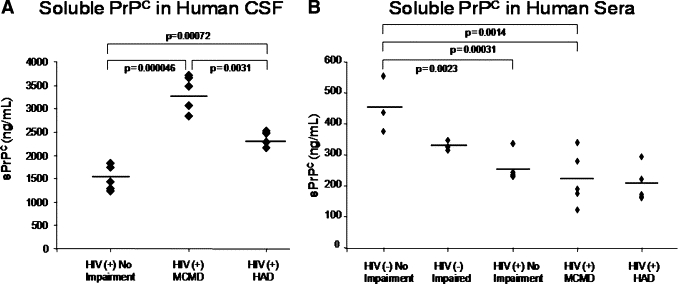
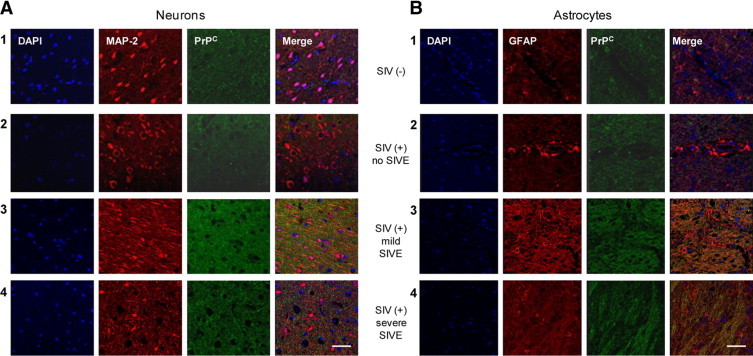
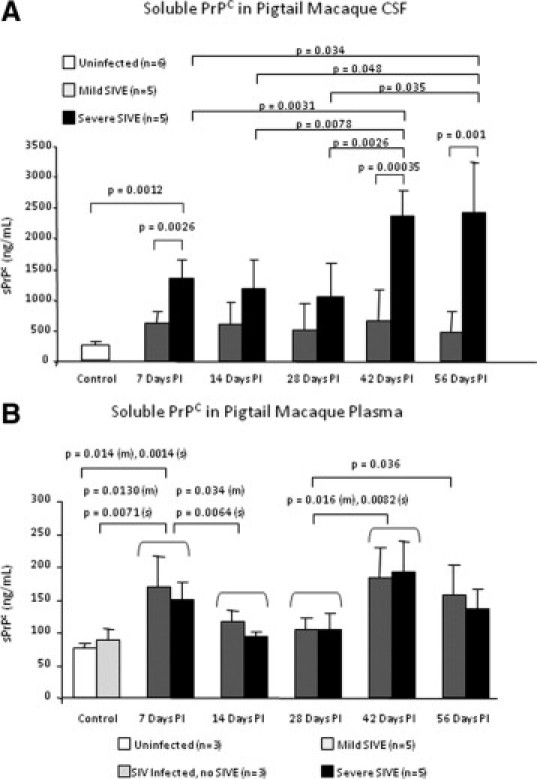
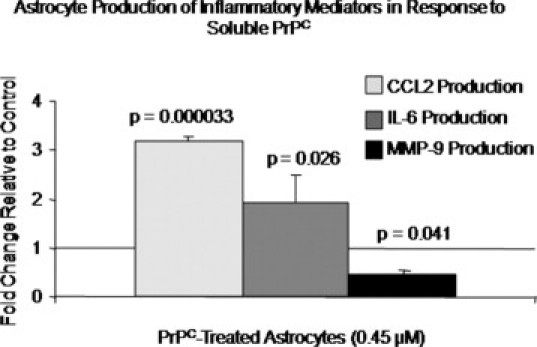
Of the 33 million people infected with the human immunodeficiency virus (HIV) worldwide, 40-60% of individuals will eventually develop neurocognitive sequelae that can be attributed to the presence of HIV-1 in the central nervous system (CNS) and its associated neuroinflammation despite antiretroviral therapy. PrP(C) (protease resistant protein, cellular isoform) is the nonpathological cellular isoform of the human prion protein that participates in many physiological processes that are disrupted during HIV-1 infection. However, its role in HIV-1 CNS disease is unknown. We demonstrate that PrP(C) is significantly increased in both the CNS of HIV-1-infected individuals with neurocognitive impairment and in SIV-infected macaques with encephalitis. PrP(C) is released into the cerebrospinal fluid, and its levels correlate with CNS compromise, suggesting it is a biomarker of HIV-associated neurocognitive impairment. We show that the chemokine (c-c Motif) Ligand-2 (CCL2) increases PrP(C) release from CNS cells, while HIV-1 infection alters PrP(C) release from peripheral blood mononuclear cells. Soluble PrP(C) mediates neuroinflammation by inducing astrocyte production of both CCL2 and interleukin 6. This report presents the first evidence that PrP(C) dysregulation occurs in cognitively impaired HIV-1-infected individuals and that PrP(C) participates in the pathogenesis of HIV-1-associated CNS disease.
Figures
References
-
- UNAIDS . Report on the global AIDS epidemic 2008. World Health Organization; Geneva: 2008.
-
- Tozzi V, Balestra P, Lorenzini P, Bellagamba R, Galgani S, Corpolongo A, Vlassi C, Larussa D, Zaccarelli M, Noto P, Visco-Comandini U, Giulianelli M, Ippolito G, Antinori A, Narciso P. Prevalence and risk factors for human immunodeficiency virus-associated neurocognitive impairment, 1996 to 2002: results from an urban observational cohort. J Neurovirol. 2005;11:265–273. - PubMed
-
- Antinori A, Arendt G, Becker JT, Brew BJ, Byrd DA, Cherner M, Clifford DB, Cinque P, Epstein LG, Goodkin K, Gisslen M, Grant I, Heaton RK, Joseph J, Marder K, Marra CM, McArthur JC, Nunn M, Price RW, Pulliam L, Robertson KR, Sacktor N, Valcour V, Wojna VE. Updated research nosology for HIV-associated neurocognitive disorders. Neurology. 2007;69:1789–1799. - PMC - PubMed
-
- van Gorp WG, Baerwald JP, Ferrando SJ, McElhiney MC, Rabkin JG. The relationship between employment and neuropsychological impairment in HIV infection. J Int Neuropsychol Soc. 1999;5:534–539. - PubMed
-
- Heaton RK, Marcotte TD, Mindt MR, Sadek J, Moore DJ, Bentley H, McCutchan JA, Reicks C, Grant I. The impact of HIV-associated neuropsychological impairment on everyday functioning. J Int Neuropsychol Soc. 2004;10:317–331. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01NS44815/NS/NINDS NIH HHS/United States
- AI071326/AI/NIAID NIH HHS/United States
- AI-051519/AI/NIAID NIH HHS/United States
- R01 MH096625/MH/NIMH NIH HHS/United States
- P01 MH070306/MH/NIMH NIH HHS/United States
- R01NS055648/NS/NINDS NIH HHS/United States
- MH076679/MH/NIMH NIH HHS/United States
- F31 AI071326/AI/NIAID NIH HHS/United States
- U01 MH083501/MH/NIMH NIH HHS/United States
- R01 MH075679/MH/NIMH NIH HHS/United States
- R01 NS055648/NS/NINDS NIH HHS/United States
- M01-RR-00071/RR/NCRR NIH HHS/United States
- R01 NS044815/NS/NINDS NIH HHS/United States
- P01MH070306/MH/NIMH NIH HHS/United States
- R24 MH059724/MH/NIMH NIH HHS/United States
- R01 MH069116/MH/NIMH NIH HHS/United States
- P30 AI051519/AI/NIAID NIH HHS/United States
- R01MH075679/MH/NIMH NIH HHS/United States
- R24MH59724/MH/NIMH NIH HHS/United States
- R01MH069116/MH/NIMH NIH HHS/United States
- M01 RR000071/RR/NCRR NIH HHS/United States
- R01 MH070297/MH/NIMH NIH HHS/United States
- U01MH083501/MH/NIMH NIH HHS/United States
- MH52974/MH/NIMH NIH HHS/United States
- K01 MH076679/MH/NIMH NIH HHS/United States
- MH070297/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
