

Intravenous thrombolysis plus hypothermia for acute treatment of ischemic stroke (ICTuS-L): final results
- PMID: 20724711
- PMCID: PMC2947593
- DOI: 10.1161/STROKEAHA.110.592295
Intravenous thrombolysis plus hypothermia for acute treatment of ischemic stroke (ICTuS-L): final results
Abstract
Background and purpose: Induced hypothermia is a promising neuroprotective therapy. We studied the feasibility and safety of hypothermia and thrombolysis after acute ischemic stroke.
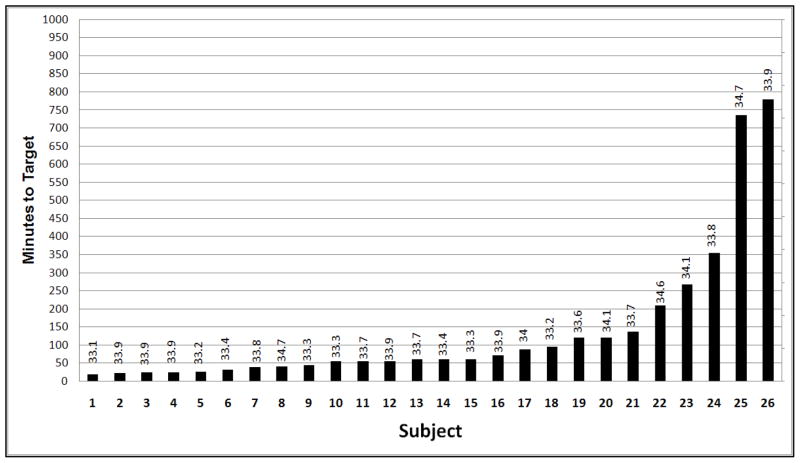
Methods: Intravenous Thrombolysis Plus Hypothermia for Acute Treatment of Ischemic Stroke (ICTuS-L) was a randomized, multicenter trial of hypothermia and intravenous tissue plasminogen activator in patients treated within 6 hours after ischemic stroke. Enrollment was stratified to the treatment time windows 0 to 3 and 3 to 6 hours. Patients presenting within 3 hours of symptom onset received standard dose intravenous alteplase and were randomized to undergo 24 hours of endovascular cooling to 33°C followed by 12 hours of controlled rewarming or normothermia treatment. Patients presenting between 3 and 6 hours were randomized twice: to receive tissue plasminogen activator or not and to receive hypothermia or not. Results- In total, 59 patients were enrolled. One patient was enrolled but not treated when pneumonia was discovered just before treatment. All 44 patients enrolled within 3 hours and 4 of 14 patients enrolled between 3 to 6 hours received tissue plasminogen activator. Overall, 28 patients randomized to receive hypothermia (HY) and 30 to normothermia (NT). Baseline demographics and risk factors were similar between groups. Mean age was 65.5±12.1 years and baseline National Institutes of Health Stroke Scale score was 14.0±5.0; 32 (55%) were male. Cooling was achieved in all patients except 2 in whom there were technical difficulties. The median time to target temperature after catheter placement was 67 minutes (Quartile 1 57.3 to Quartile 3 99.4). At 3 months, 18% of patients treated with hypothermia had a modified Rankin Scale score of 0 or 1 versus 24% in the normothermia groups (nonsignificant). Symptomatic intracranial hemorrhage occurred in 4 patients (68); all were treated with tissue plasminogen activator <3 hours (1 received hypothermia). Six patients in the hypothermia and 5 in the normothermia groups died within 90 days (nonsignificant). Pneumonia occurred in 14 patients in the hypothermia and in 3 of the normothermia groups (P=0.001). The pneumonia rate did not significantly adversely affect 3 month modified Rankin Scale score (P=0.32).
Conclusions: This study demonstrates the feasibility and preliminary safety of combining endovascular hypothermia after stroke with intravenous thrombolysis. Pneumonia was more frequent after hypothermia, but further studies are needed to determine its effect on patient outcome and whether it can be prevented. A definitive efficacy trial is necessary to evaluate the efficacy of therapeutic hypothermia for acute stroke.
Figures
References
-
- O’Collins VE, Macleod MR, Donnan GA, Horky LL, van der Worp BH, Howells DW. 1,026 experimental treatments in acute stroke. Ann Neurol. 2006;59(3):467–77. - PubMed
-
- Popovic R, Liniger R, Bickler PE. Anesthetics and mild hypothermia similarly prevent hippocampal neuron death in an in vitro model of cerebral ischemia. Anesthesiology. 2000;92(5):1343–9. - PubMed
-
- Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346(8):557–63. - PubMed
-
- The Hypothermia After Cardiac Arrest Study G. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346(8):549–56. - PubMed
-
- Nolan JP, Morley PT, Vanden Hoek TL, Hickey RW, Kloeck WG, Billi J, et al. Therapeutic hypothermia after cardiac arrest: an advisory statement by the advanced life support task force of the International Liaison Committee on Resuscitation. Circulation. 2003;108(1):118–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
