

A review of acne in ethnic skin: pathogenesis, clinical manifestations, and management strategies
- PMID: 20725545
- PMCID: PMC2921746
A review of acne in ethnic skin: pathogenesis, clinical manifestations, and management strategies
Abstract
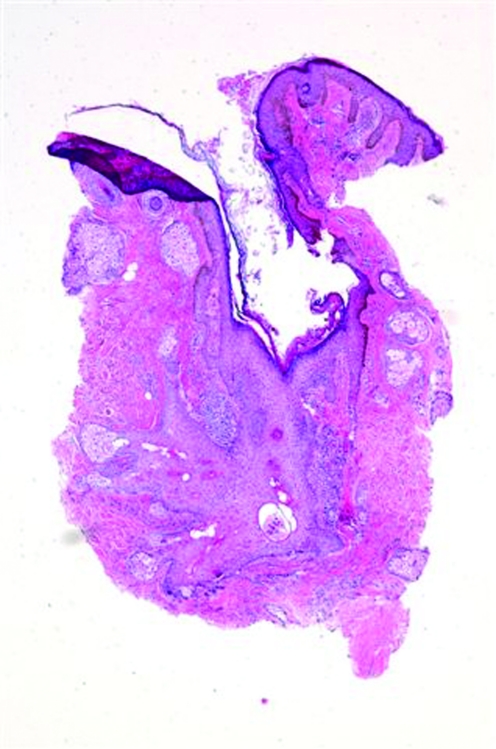
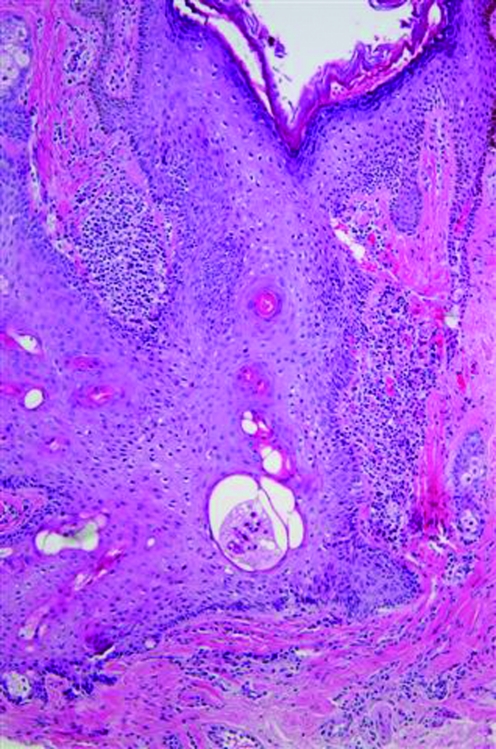
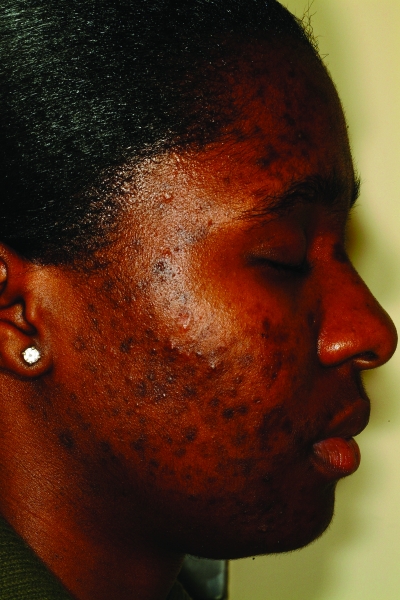
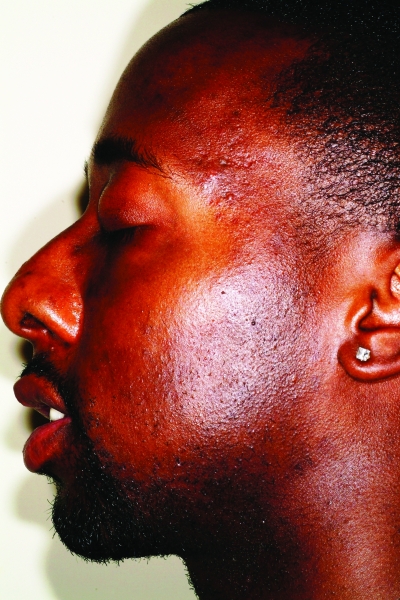
Acne vulgaris is one of the most common conditions for which all patients, including those with skin of color (Fitzpatrick skin types IV-VI), seek dermatological care. The multifactorial pathogenesis of acne appears to be the same in ethnic patients as in Caucasians. However, there is controversy over whether certain skin biology characteristics, such as sebum production, differ in ethnic patients. Clinically, acne lesions can appear the same as those seen in Caucasians; however, histologically, all types of acne lesions in African Americans can be associated with intense inflammation including comedones, which can also have some degree of inflammation. It is the sequelae of the disease that are the distinguishing characteristics of acne in skin of color, namely postinflammatory hyperpigmentation and keloidal or hypertrophic scarring. Although the medical and surgical treatment options are the same, it is these features that should be kept in mind when designing a treatment regimen for acne in skin of color.
Figures














References
-
- White GM. Recent findings in the epidemiologic evidence, classification, and subtypes of acne vulgaris. J Am Acad Dermatol. 1998;39:S34–S37. - PubMed
-
- Alexis AF, Sergay AB, Taylor SC. Common dermatologic disorders in skin of color: a comparative practice survey. Cutis. 2007;80:38–394. - PubMed
-
- Fox H. Observations on skin diseases in the Negro. J Cutan Dis. 1908;26:67–79.
-
- Hazen HH. Personal observations upon skin diseases in the American Negro. J Cutan Dis. 1914;32:705–712.
-
- Hazen HH. Syphilis and skin disease in the American Negro: personal observations. AMA Arch Derm Syphilol. 1935;31:316–323.
LinkOut - more resources
Full Text Sources