

Pioglitazone attenuates prostatic enlargement in diet-induced insulin-resistant rats by altering lipid distribution and hyperinsulinaemia
- PMID: 20726985
- PMCID: PMC3010577
- DOI: 10.1111/j.1476-5381.2010.00994.x
Pioglitazone attenuates prostatic enlargement in diet-induced insulin-resistant rats by altering lipid distribution and hyperinsulinaemia
Abstract
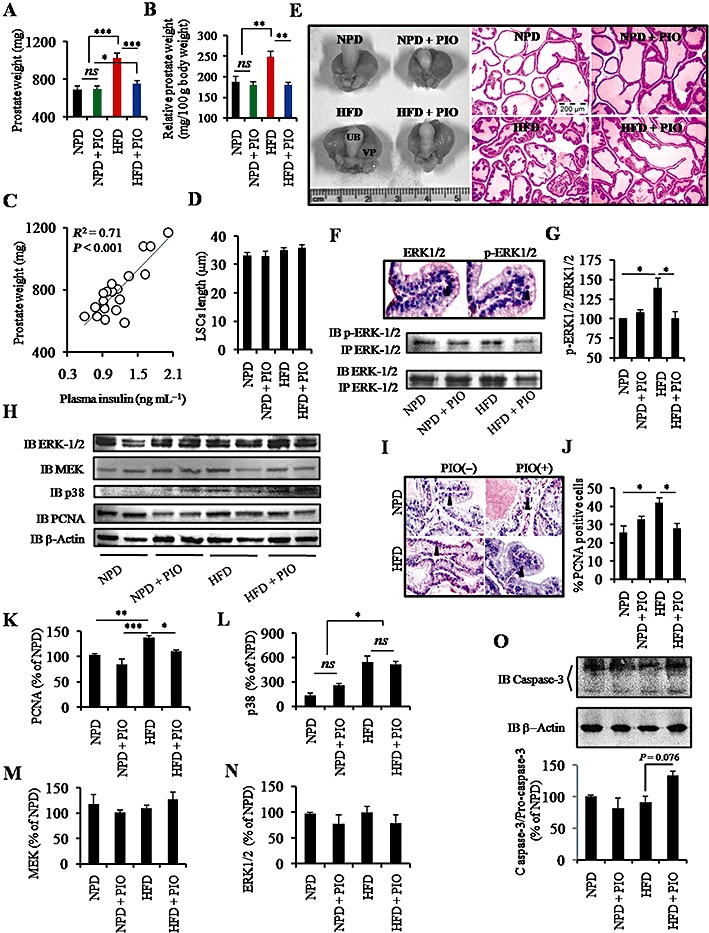
Background and purpose: Increased incidence of benign prostatic hyperplasia among insulin-resistant individuals suggests a role for hyperinsulinaemia in prostatic enlargement. We have already reported increased cell proliferation and enlargement of prostate gland in insulin-resistant rats. The present study aimed to elucidate the molecular mechanisms underlying the reversal of prostatic enlargement in insulin-resistant rats by the peroxisome proliferator-activated receptor γ agonist pioglitazone.
Experimental approach: Sprague-Dawley rats were fed a normal pellet or a high-fat diet for 12 weeks with or without pioglitazone (20 mg·kg(-1)). Subgroups of animals fed different diets were castrated. Effects of dietary manipulation and pioglitazone were measured on insulin sensitivity, lipid distribution, cell proliferation and apoptosis.
Key results: A high-fat diet led to the accumulation of fat in non-adipose tissues, insulin resistance, compensatory hyperinsulinaemia and prostatic enlargement in rats. Pioglitazone treatment altered fat distribution, improved insulin sensitivity and normalized lipid and insulin level in rats on the high-fat diet. The improved metabolic parameters led to decreased cellular proliferation and increased apoptosis in the prostate gland. High-fat diet feeding and pioglitazone treatment did not change plasma testosterone levels. However, significant prostatic atrophy was observed in castrated rats irrespective of dietary intervention.
Conclusions and implications: Our results show a previously unexplored therapeutic potential of pioglitazone for prostatic enlargement under insulin-resistant condition and further suggest that targeting distribution of lipid from non-adipose tissue to adipose tissue and insulin signalling could be new strategies for the treatment of benign prostatic hyperplasia.
© 2010 The Authors. British Journal of Pharmacology © 2010 The British Pharmacological Society.
Figures






Comment in
-
Re: Pioglitazone attenuates prostatic enlargement in diet-induced insulin-resistant rats by altering lipid distribution and hyperinsulinaemia.J Urol. 2011 Dec;186(6):2496-7. doi: 10.1016/j.juro.2011.08.035. Epub 2011 Oct 22. J Urol. 2011. PMID: 22078628 No abstract available.
References
-
- Attia N, Tamborlane WV, Heptulla R, Maggs D, Grozman A, Sherwin RS, et al. The metabolic syndrome and insulin-like growth factor I regulation in adolescent obesity. J Clin Endocrinol Metab. 1998;83:1467–1471. - PubMed
-
- Berry SJ, Coffey DS, Walsh PC, Ewing LL. The development of human benign prostatic hyperplasia with age. J Urol. 1984;132:474–479. - PubMed
-
- Cai X, Haleem R, Oram S, Cyriac J, Jiang F, Grayhack JT, et al. High fat diet increases the weight of rat ventral prostate. Prostate. 2001;49:1–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
