

Carotid intima-media thickness in individuals with and without type 2 diabetes: a reproducibility study
- PMID: 20727128
- PMCID: PMC2931499
- DOI: 10.1186/1475-2840-9-40
Carotid intima-media thickness in individuals with and without type 2 diabetes: a reproducibility study
Abstract
Background: The use of carotid intima-media thickness (carotid IMT) as a surrogate marker of cardiovascular disease is increasing and the method has now also been applied in several trials investigating patients with type 2 diabetes (T2D). Even though knowledge about methodology is of highest importance in order to make accurate power calculations and analyses of results, no reproducibility studies have been performed in this group of patients. The aim of this study was to quantify the variability of the measurement of carotid IMT in individuals with and without T2D.
Methods: We used B-mode ultrasound and a computerized software programme (MIA vascular tools) for analysis of carotid IMT. Measurement of carotid IMT in the far wall of the common carotid artery (CCA) was done for 30 patients with T2D and 30 persons without T2D. The examinations were done by two different sonographers and two different readers on two separate days in order to quantify sonographer-, reader-, and day-to-day variability.
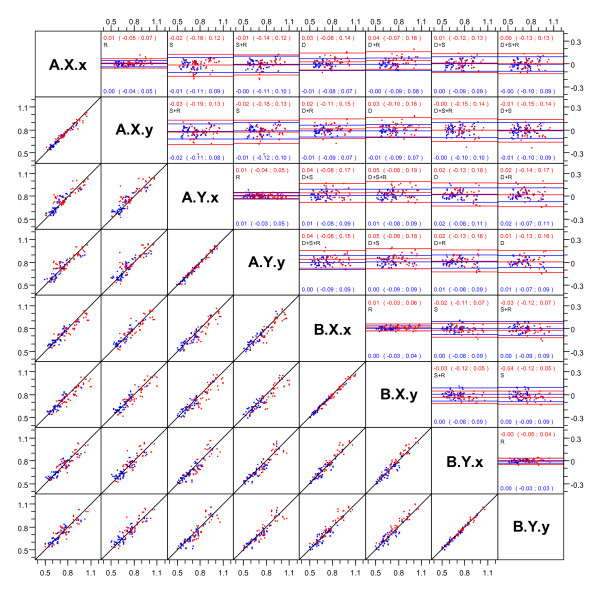
Results: Comparisons of measurement of carotid IMT in CCA between sonographers (sonographer variability) resulted in limits of agreement (LoA) from -0.18 to 0.13 mm for patients with T2D and -0.12 to 0.10 mm for persons without T2D. This means, that a second scanning of the same person with 95% probability would be within this interval of the first scanning. Comparisons between readers assessing the same scanning (reader variability) resulted in LoA from -0.05 to 0.07 mm and -0.04 to 0.05 mm respectively. LoA of the day-to-day variability was -0.13 to 0.18 mm and -0.09 to 0.18 mm respectively. This corresponds to coefficients of variations (CV) of the sonographer- and day-to-day variability of 10% in patients with T2D and 8% in persons without T2D. The CV of the reader variability was 4% and 3% respectively.
Conclusion: Measurement of carotid IMT in the CCA can be determined with good and comparable reproducibility in both patients with T2D and persons without T2D. These findings support the use of carotid IMT in clinical trials with T2D patients and suggest that the numbers of patients needed to detect a given difference will be the same whether the patients have T2D or not.
Figures
Similar articles
-
Measurement of common carotid artery intima-media thickness in clinical practice: comparison of B-mode and RF-based technique.Ultraschall Med. 2009 Oct;30(5):459-65. doi: 10.1055/s-0028-1109187. Epub 2009 Jun 18. Ultraschall Med. 2009. PMID: 19544231
-
Multi-examiner reliability of automated radio frequency-based ultrasound measurements of common carotid intima-media thickness in rheumatoid arthritis.Rheumatology (Oxford). 2011 Oct;50(10):1860-4. doi: 10.1093/rheumatology/ker206. Epub 2011 Jun 29. Rheumatology (Oxford). 2011. PMID: 21719420
-
Noninvasive measurement of carotid extra-media thickness: associations with cardiovascular risk factors and intima-media thickness.JACC Cardiovasc Imaging. 2009 Feb;2(2):176-82. doi: 10.1016/j.jcmg.2008.09.013. JACC Cardiovasc Imaging. 2009. PMID: 19356553
-
Reproducibility of in vivo carotid intima-media thickness measurements: a review.Stroke. 1997 Mar;28(3):665-71. doi: 10.1161/01.str.28.3.665. Stroke. 1997. PMID: 9056629 Review.
-
Mannheim carotid intima-media thickness consensus (2004-2006). An update on behalf of the Advisory Board of the 3rd and 4th Watching the Risk Symposium, 13th and 15th European Stroke Conferences, Mannheim, Germany, 2004, and Brussels, Belgium, 2006.Cerebrovasc Dis. 2007;23(1):75-80. doi: 10.1159/000097034. Epub 2006 Nov 14. Cerebrovasc Dis. 2007. PMID: 17108679
Cited by
-
Intervendor variability of carotid intima-media thickness measurement: validation study using newly developed ultrasound phantom.J Med Ultrason (2001). 2020 Apr;47(2):155-165. doi: 10.1007/s10396-019-00995-7. Epub 2020 Feb 17. J Med Ultrason (2001). 2020. PMID: 32067178
-
Long-term effects of different hypoglycemic drugs on carotid intima-media thickness progression: a systematic review and network meta-analysis.Front Endocrinol (Lausanne). 2024 May 31;15:1403606. doi: 10.3389/fendo.2024.1403606. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38883606 Free PMC article.
-
GCKR gene functional variants in type 2 diabetes and metabolic syndrome: do the rare variants associate with increased carotid intima-media thickness?Cardiovasc Diabetol. 2010 Nov 29;9:79. doi: 10.1186/1475-2840-9-79. Cardiovasc Diabetol. 2010. PMID: 21114848 Free PMC article.
-
Dynamic changes of carotid artery intima-media thickness and mortality in hemodialysis patients.Hippokratia. 2015 Apr-Jun;19(2):158-63. Hippokratia. 2015. PMID: 27418766 Free PMC article.
-
Increased serum myeloid-related protein 8/14 level is associated with atherosclerosis in type 2 diabetic patients.Cardiovasc Diabetol. 2011 May 18;10:41. doi: 10.1186/1475-2840-10-41. Cardiovasc Diabetol. 2011. PMID: 21592353 Free PMC article.
References
-
- Bots ML, Hoes AW, Koudstaal PJ, Hofman A, Grobbee DE. Common carotid intima-media thickness and risk of stroke and myocardial infarction: the Rotterdam Study. Circulation. 1997;96:1432–1437. - PubMed
-
- Chambless LE, Folsom AR, Clegg LX, Sharrett AR, Shahar E, Nieto FJ, Rosamond WD, Evans G. Carotid wall thickness is predictive of incident clinical stroke: the Atherosclerosis Risk in Communities (ARIC) study. American Journal of Epidemiology. 2000;151:478–487. - PubMed
-
- O'Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, Wolfson SK Jr. Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. Cardiovascular Health Study Collaborative Research Group. N Engl J Med. 1999;340:14–22. doi: 10.1056/NEJM199901073400103. - DOI - PubMed
-
- Yamasaki Y, Kodama M, Nishizawa H, Sakamoto K, Matsuhisa M, Kajimoto Y, Kosugi K, Shimizu Y, Kawamori R, Hori M. Carotid intima-media thickness in Japanese type 2 diabetic subjects: predictors of progression and relationship with incident coronary heart disease. Diabetes Care. 2000;23:1310–1315. doi: 10.2337/diacare.23.9.1310. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
