

Significance of lobular intraepithelial neoplasia at margins of breast conservation specimens: a report of 38 cases and literature review
- PMID: 20727142
- PMCID: PMC2936385
- DOI: 10.1186/1746-1596-5-54
Significance of lobular intraepithelial neoplasia at margins of breast conservation specimens: a report of 38 cases and literature review
Abstract
Background: Presence of lobular intraepithelial neoplasia (LIN) is not routinely reported as part of margin assessment in breast conservation therapy (BCT) as in ductal carcinoma in situ (DCIS). With new emerging evidence of LIN as possible precursor lesion, the hypothesis is that LIN at the margin may increase the risk of local recurrence with BCT. The aim is to determine whether there is an increase incidence of recurrence when LIN is found at surgical margins on BCT.
Methods: We retrospectively reviewed a total of 1,334 BCT at a single institution in a 10 year period. Inclusion criteria are positive margin with LIN from primary BCT containing invasive and/or in situ carcinoma with comparison to the negative control group who had similar diseases with negative margin for LIN.
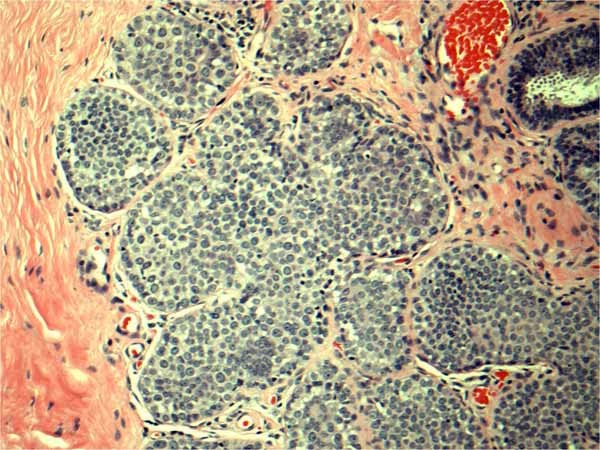
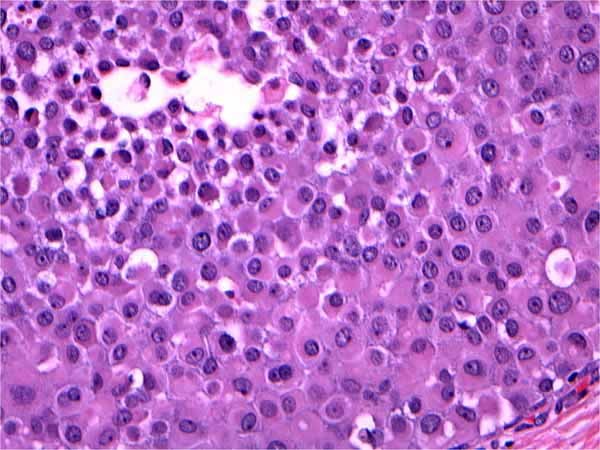
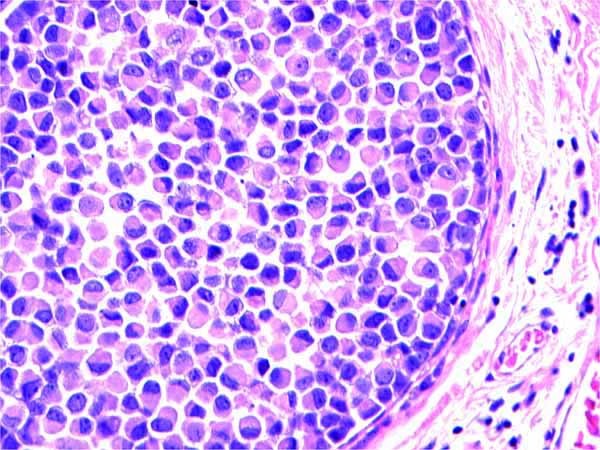
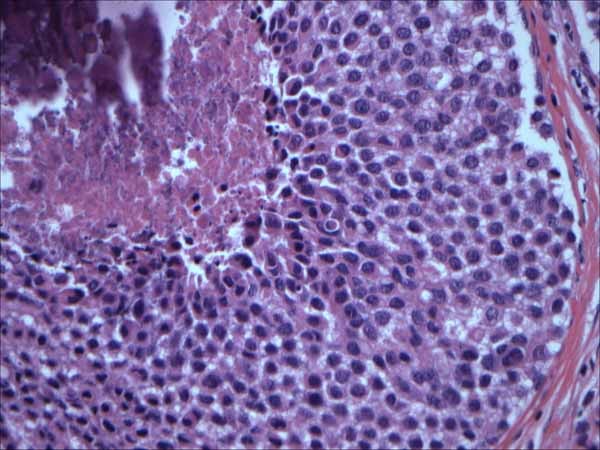
Results: We identified 38 cases (2.8%) with LIN either lobular carcinoma in situ/atypical lobular hyperplasia (LCIS/ALH) at a margin on initial BCT with 36% recurrence rate. Of the 38 cases: 5 (13%) were lost to follow-up, 12 (32%) had no further procedures performed and 21 (55%) had re-excision. Out of 21 patients who had re-excisions, 12 (57%) had residual invasive carcinoma or DCIS, three (14%) had pleomorphic LCIS and 4 (19%) showed residual classic type LCIS. 71% had significant residual disease (local recurrence) and 29% had no residual disease. A negative control group consisted of 38 cases. We found two patients with bone or brain metastasis and one local recurrence. Clinical follow up periods range from 1 to 109 months.
Conclusions: LIN found at a margin on BCT showed a significant recurrent ipsilateral disease. Our study supports the view that LIN seen at the margin may play a role in recurrence.
Figures

References
-
- Haagensen CD, Lane N, Lattes R. Lobular neoplasia (so called lobular carcinoma in situ) of the breast. Cancer. 1978;42:1024–34. - PubMed
-
- De Leeuw W, Berx G, Vos C, Peterse JL, Van de Vijver MJ, Litvinov S, Van Roy F, Cornelisse CJ, Cleton-Jansen AM. Simultaneous loss of E-cadherin and catenins in invasive lobular breast cancer and lobular carcinoma in situ. J Pathol. 1997;183:404–11. doi: 10.1002/(SICI)1096-9896(199712)183:4<404::AID-PATH1148>3.0.CO;2-9. - DOI - PubMed
