

Outcomes associated with phosphorus binders in men with non-dialysis-dependent CKD
- PMID: 20728255
- PMCID: PMC2963702
- DOI: 10.1053/j.ajkd.2010.06.011
Outcomes associated with phosphorus binders in men with non-dialysis-dependent CKD
Abstract
Background: Phosphorus binders are used to treat hyperphosphatemia in maintenance dialysis patients, in whom the use of these medications has been associated with lower mortality in some observational studies. It is not clear whether similar benefits can be seen in patients with non-dialysis-dependent chronic kidney disease (CKD).
Study design: Historical cohort.
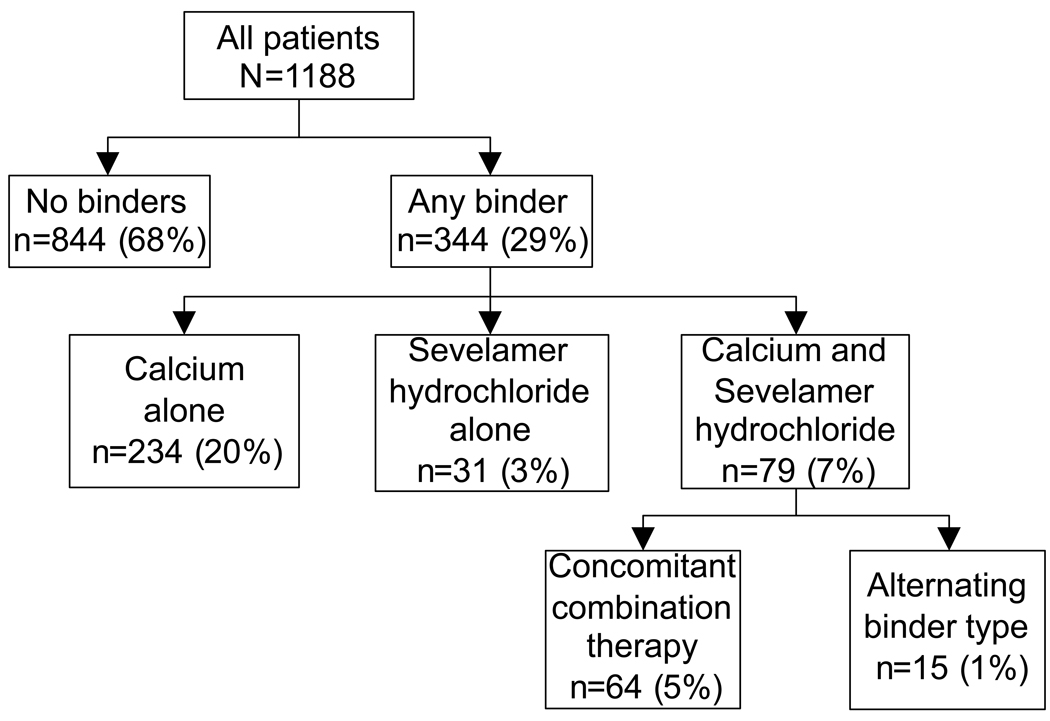
Setting & participants: 1,188 men with moderate and advanced non-dialysis-dependent CKD at a single medical center.
Predictor: Administration of any phosphorus binder.
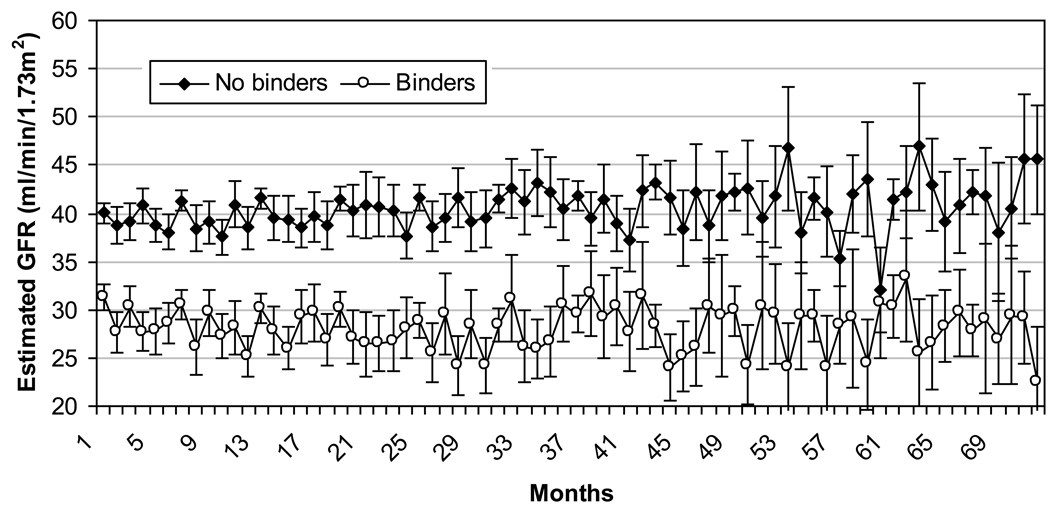
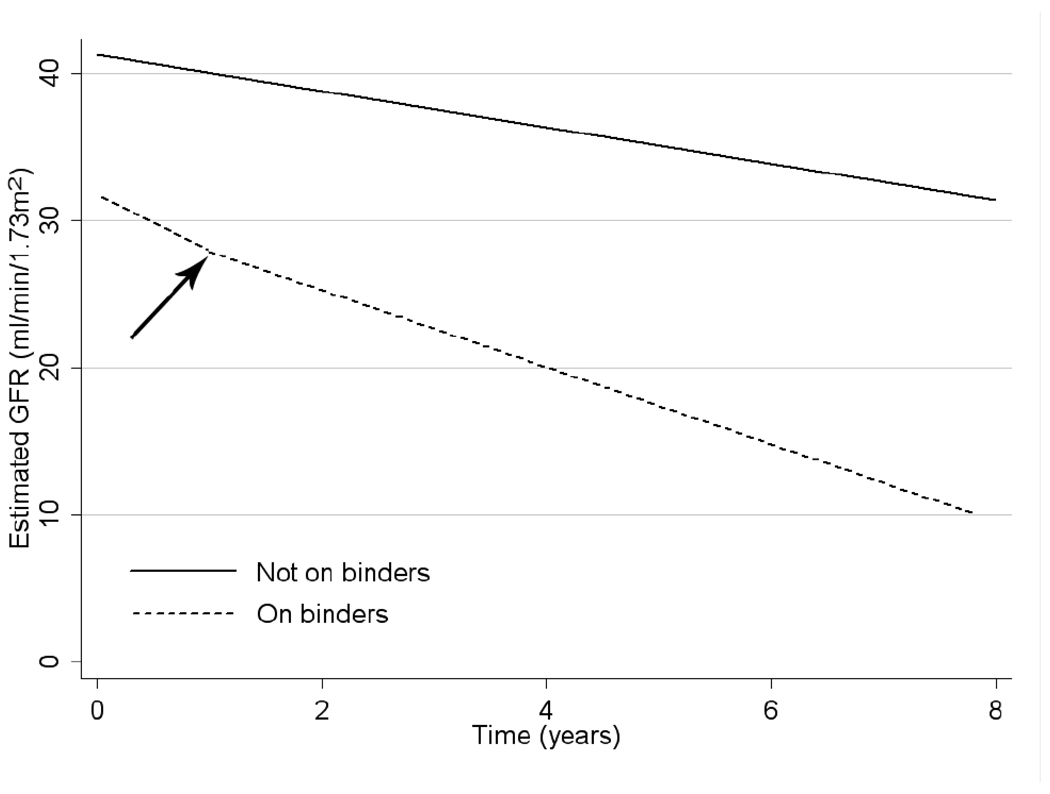
Outcomes & measurements: We examined associations of any phosphorus-binder administration with all-cause mortality and the slopes of estimated glomerular filtration rate using time-varying Cox models and mixed-effects models. Associations also were examined in intention-to-treat analyses and in 133 patient-pairs matched according to propensity scores.
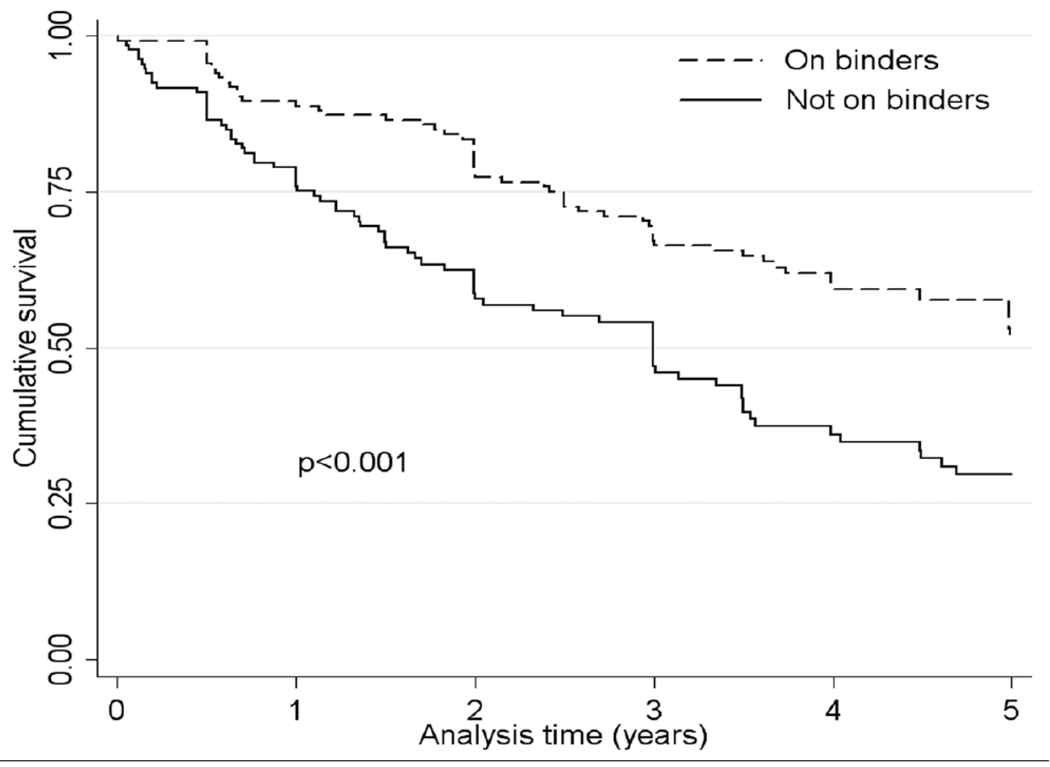
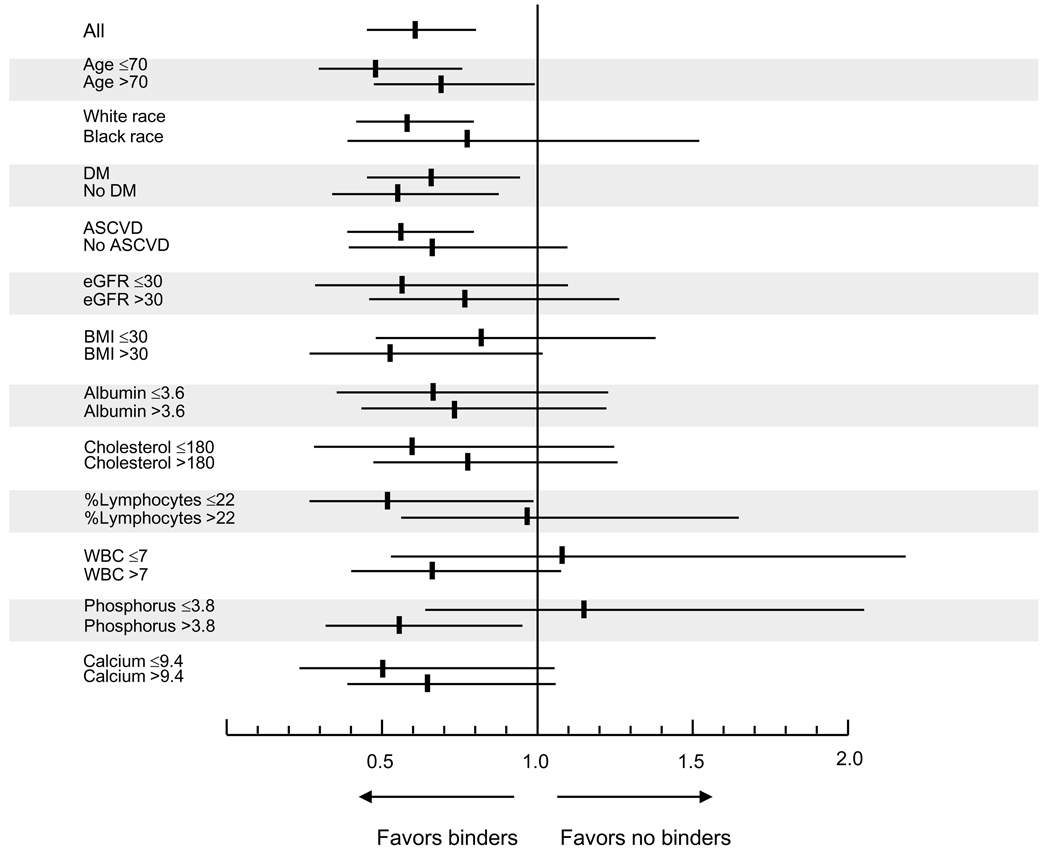
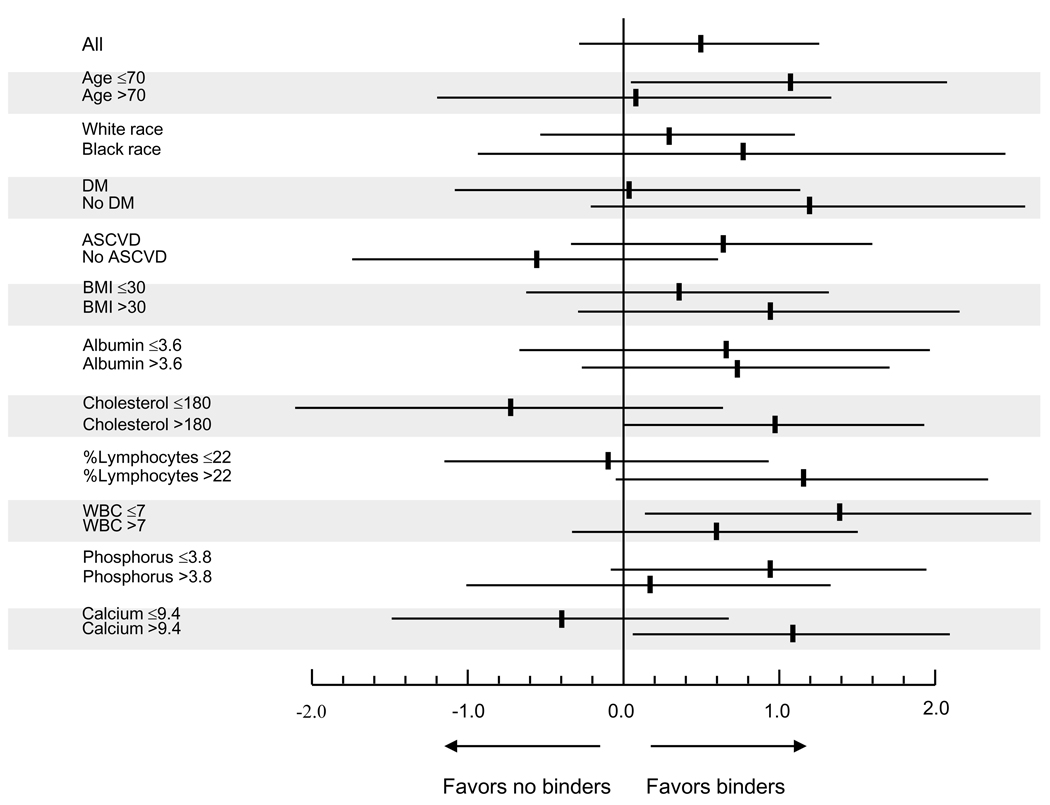
Results: 344 patients were treated with a phosphorus binder; 658 patients died (mortality rate, 141 deaths/1,000 patient-years; 95% CI, 131-153) during a median follow-up of 3.1 years. Treatment with phosphorus binders was associated with significantly lower mortality (adjusted HR, 0.61; 95% CI, 0.45-0.81; P < 0.001). Results were similar when exposure was modeled in intention-to-treat analyses and examining propensity-matched patients. Phosphorus-binder use was not associated with significant changes in kidney function loss.
Limitations: Results may not apply to all patients with non-dialysis-dependent CKD.
Conclusions: Administration of phosphorus binders is associated with lower mortality in men with moderate and advanced non-dialysis-dependent CKD. Clinical trials are needed to determine the risks and benefits of phosphorus-binder use in this patient population.
Published by Elsevier Inc.
Figures
Comment in
-
Off-label use of phosphate binders in non-dialysis-dependent CKD.Am J Kidney Dis. 2010 Nov;56(5):813-6. doi: 10.1053/j.ajkd.2010.09.004. Am J Kidney Dis. 2010. PMID: 20970022 No abstract available.
References
-
- Kovesdy CP, Kalantar-Zadeh K. Bone and mineral disorders in pre-dialysis CKD. Int Urol Nephrol. 2008;40:427–440. - PubMed
-
- Block GA, Klassen PS, Lazarus JM, Ofsthun N, Lowrie EG, Chertow GM. Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. J Am Soc Nephrol. 2004;15:2208–2218. - PubMed
-
- Kalantar-Zadeh K, Kuwae N, Regidor DL, et al. Survival predictability of time-varying indicators of bone disease in maintenance hemodialysis patients. Kidney Int. 2006;70:771–780. - PubMed
-
- Slinin Y, Foley RN, Collins AJ. Calcium, phosphorus, parathyroid hormone, and cardiovascular disease in hemodialysis patients: the USRDS waves 1, 3, and 4 study. J Am Soc Nephrol. 2005;16:1788–1793. - PubMed
-
- Tentori F, Blayney MJ, Albert JM, et al. Mortality risk for dialysis patients with different levels of serum calcium, phosphorus, and PTH: the Dialysis Outcomes and Practice Patterns Study (DOPPS) Am J Kidney Dis. 2008;52:519–530. - PubMed
