

Mind the gap
- PMID: 20729177
- PMCID: PMC3002182
- DOI: 10.1289/ehp.1002517
Mind the gap
Abstract
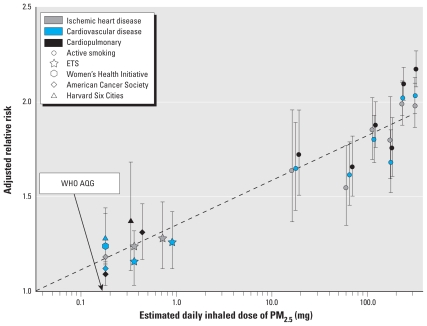
Background: Recent analysis has demonstrated a remarkably consistent, nonlinear relationship between estimated inhaled dose of combustion particles measured as PM(2.5) (particulate matter with aerodynamic diameter ≤ 2.5 µm) and cardiovascular disease mortality over several orders of magnitude of dose--from cigarette smoking, environmental tobacco smoke (ETS) exposure, and ambient air pollution exposure.
Objectives: Here we discuss the implications of this relationship and point out the gaps in our knowledge that it reveals.
Discussion: The nonlinear exposure-response relationship that is revealed-much steeper at lower than at higher doses-explains the seemingly inconsistent risks observed from ambient air pollution and cigarette smoking but also raises important questions about the relative benefits of control at different points along the curve. This analysis also reveals a gap in the evidence base along the dose-response curve between ETS and active smoking, which is the dose range experienced by half the world's population from indoor biomass and coal burning for cooking and heating.
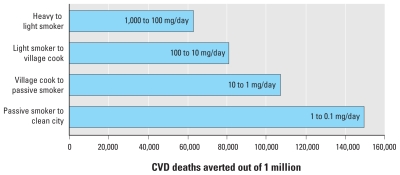
Conclusions: The shape of the exposure-response relationship implies much larger public health benefits of reductions at the lower end of the dose spectrum (e.g., from reductions in outdoor air pollution) than from reducing the rate of active smoking, which seems counterintuitive and deserving of further study because of its importance for control policies. In addition, given the potential risks and consequent global disease burden, epidemiologic studies are urgently needed to quantify the cardiovascular risks of particulate matter exposures from indoor biomass burning in developing countries, which lie in the dose gap of current evidence.
Figures
Comment in
-
A break in the continuum: analyzing the gap in particle exposure research.Environ Health Perspect. 2010 Dec;118(12):a543. doi: 10.1289/ehp.118-a543b. Environ Health Perspect. 2010. PMID: 21123142 Free PMC article. No abstract available.
References
-
- Ambrose JA, Barua RS. The pathophysiology of cigarette smoking and cardiovascular disease. J Am Coll Cardiol. 2004;43:1731–1737. - PubMed
-
- Barnoya J, Glantz SA. Cardiovascular effects of secondhand smoke. Nearly as large as smoking. Circulation. 2005;111:2684–2698. - PubMed
-
- Cohen AJ, Anderson HR, Ostro B, Pandey KD, Krzyzanowski M, Kuenzli N, et al. Mortality impacts of urban air pollution. In: Ezzati M, Rodgers AD, Lopez AD, Murray CJL, editors. Comparative Quantification of Health Risks: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors. Vol. 2. Geneva: World Health Organization; 2004. pp. 1353–1433.
-
- Dockery DW, Pope CA, III, Xu X, Spengler JD, Ware JH, Fay ME, et al. An association between air pollution and mortality in six U.S. cities. N Engl J Med. 1993;329:1753–1759. - PubMed
-
- Gambrose JF, Nicolich MJ. Comparison of ambient PM risks estimated from PM components of smoking and occupational exposures. J Air Waste Manag Assoc. 2000;50:1514–1531. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
