

Sarcomatoid (spindle cell) carcinoma of the head and neck mucosal region: a clinicopathologic review of 103 cases from a tertiary referral cancer centre
- PMID: 20730609
- PMCID: PMC2996502
- DOI: 10.1007/s12105-010-0204-4
Sarcomatoid (spindle cell) carcinoma of the head and neck mucosal region: a clinicopathologic review of 103 cases from a tertiary referral cancer centre
Abstract
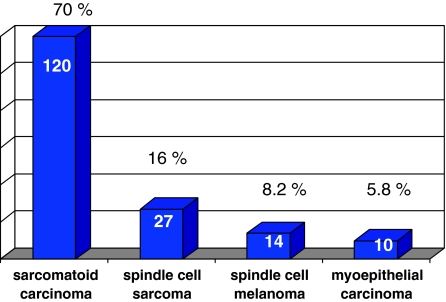
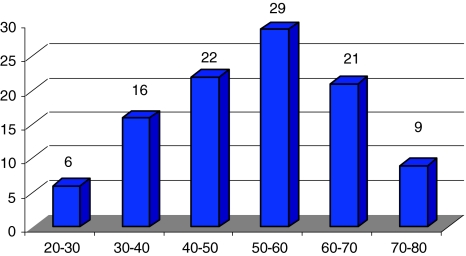
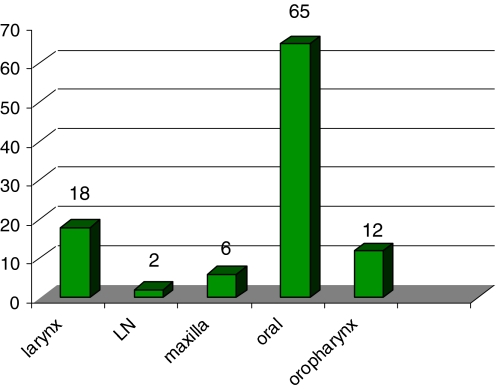
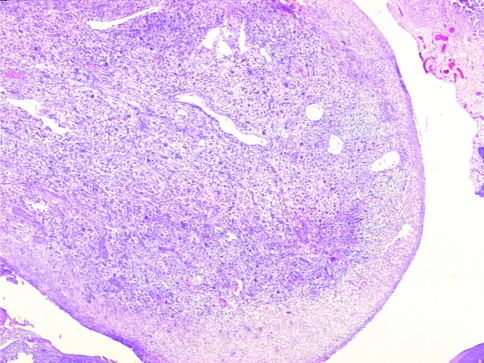
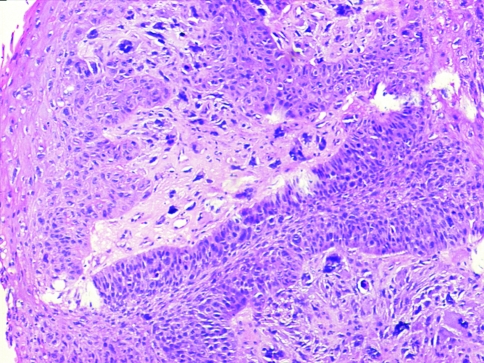
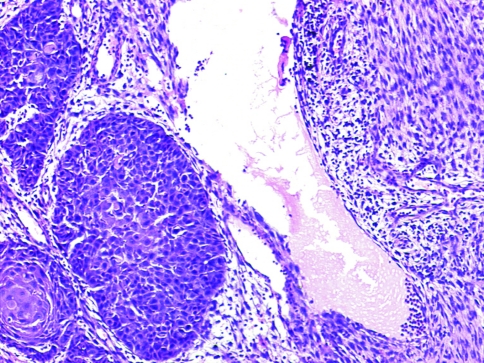
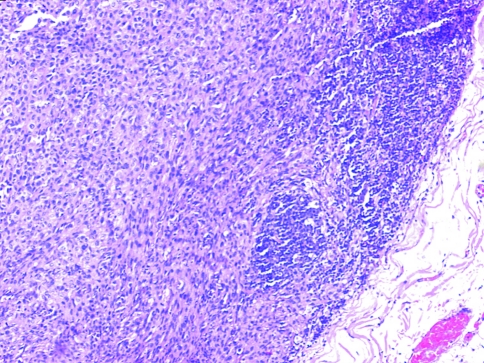
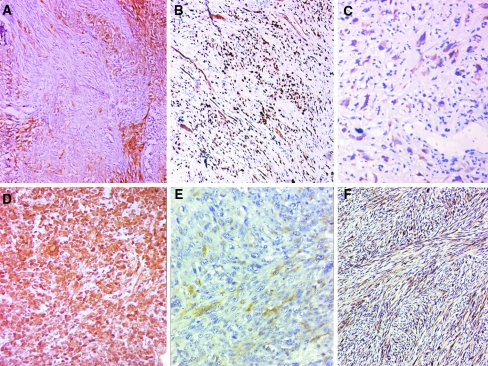
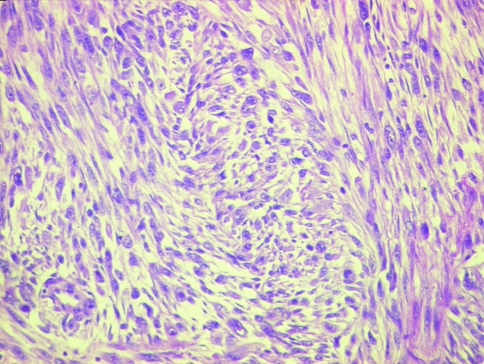
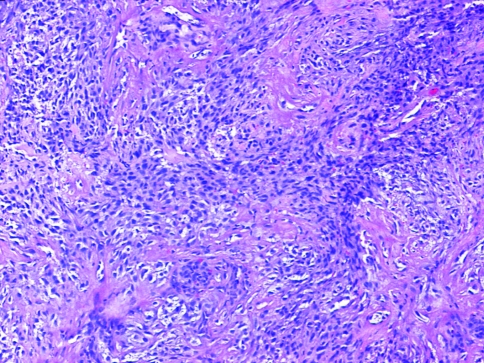
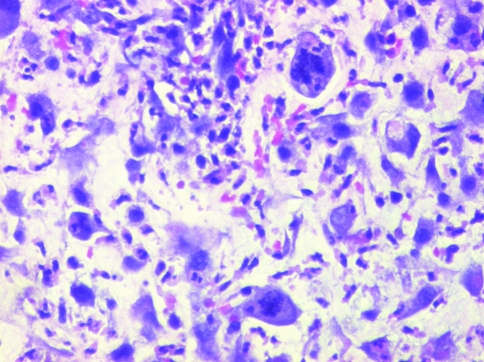
Sarcomatoid carcinomas are biphasic tumors proven to be monoclonal dedifferentiated forms of conventional squamous carcinomas. This study evaluates their clinicopathologic characteristics in head and neck mucosal sites and the problems in distinguishing them from other spindle cell tumors. A total of 103 cases with a confirmed diagnosis of sarcomatoid carcinoma accessioned in the pathology department of a tertiary referral cancer centre over a period of 7 years (2004-2010) were studied. An algorithm used for their diagnosis is presented. Ages of the patients were 22-90 years (median 53 years), and male:female ratio was 3.7:1. Site distribution was oral cavity (n = 65, 63.1%), larynx (18, 17.5%), oropharynx/hypopharynx (12, 10.7%), maxilla (6, 5.8%) and metastatic nodes (2, 1.9%). A large number of patients (95%) presented with a mass lesion of less than 1 year duration. Histopathologically, epithelial differentiation was evident on morphology in 48 (46.6%) cases, only on IHC in 34 (33%) cases, and in 21 (20.4%) no epithelial differentiation was seen. Typically, tumors were polypoidal (92, 89.3%) and ulcerated (95, 92.2%) with cells arranged predominantly in fascicles (59, 57.3%) or storiform pattern (17, 16.5%) amidst collagenous (50, 48.5%) or myxoid matrix (35, 34%). Anaplasia (2+/3+) and mitosis >10 per 10 HPF were noted in 96 (93.2%) cases. IHC was done in 82 cases; 55 (66.7%) showed positivity for epithelial markers with aberrant expression of mesenchymal markers in 43 (41.7%). Diagnosis of sarcomatoid squamous carcinoma is challenging because of overlapping histopathological features with other spindle cell tumors. Understanding their clinicopathologic characteristics facilitates their diagnosis and appropriate clinical management.
Figures


References
-
- Anderson CE, Al-Nafussi A. Spindle cell lesions of the head and neck: an overview and diagnostic approach. Diagn Histopathol. 2009;15(5):264–272. doi: 10.1016/j.mpdhp.2009.02.009. - DOI
-
- Thompson LDR. Squamous cell carcinoma variants of the head and neck. Curr Diagn Pathol. 2003;9:384–396. doi: 10.1016/S0968-6053(03)00069-3. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
