

Global genomic and RNA profiles for novel risk stratification of neuroblastoma
- PMID: 20731666
- PMCID: PMC11159775
- DOI: 10.1111/j.1349-7006.2010.01681.x
Global genomic and RNA profiles for novel risk stratification of neuroblastoma
Abstract
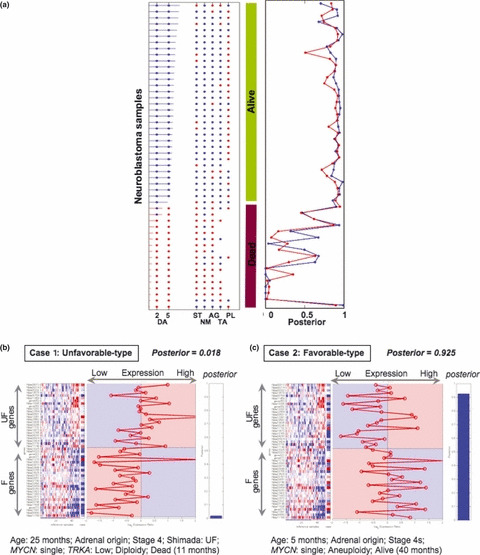
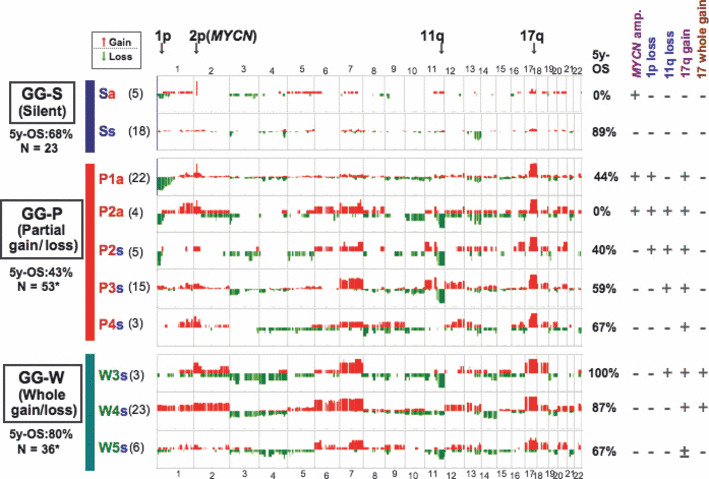
Neuroblastoma is one of the most common solid tumors in children. Its clinical behavior ranges widely from spontaneous regression to life-threatening aggressive growth. The molecular etiology of neuroblastoma is still enigmatic and the overall cure rate of advanced disease is still very poor. Recent microarray-based technology provided us with important information such as comprehensive genomic alterations and gene expression profiles to help us understand the molecular characteristics of each tumor in detail. Several retrospective studies have revealed that these signatures are strongly correlated with patient prognoses and led to the construction of new risk stratification systems, some of which are considered for evaluation in upcoming clinical studies in a prospective way. Large-scale analyses using a variety of genetic tools also discovered a major familial neuroblastoma predisposition gene ALK, as well as new candidate susceptibility genes at 6q22 and 2q35 for sporadic neuroblastoma. Of note, ALK is mutated in 6-9% of sporadic cases, and is either amplified or constitutively activated through mutations mainly within the kinase domain, promoting the possibility of new therapeutic strategies using ALK inhibitors. Additional candidates for outcome predictors such as the methylation phenotype of tumor DNA and expression profiles of microRNA have also been proposed. Such variety of information will help us understand the heterogeneity of neuroblastoma biology and further, the combined use of these signatures will be beneficial in predicting prognosis with high accuracy, as well as choosing a suitable therapy for the individual patient.
© 2010 Japanese Cancer Association.
Figures
References
-
- Brodeur GM. Neuroblastoma: biological insight into a clinical enigma. Nat Rev Cancer 2003; 3: 203–16. - PubMed
-
- Maris JM. The biologic basis for neuroblastoma heterogeneity and risk stratification. Curr Opin Pediatr 2005; 17: 7–13. - PubMed
-
- Look AT, Hayes FA, Nitschke R, McWilliams NB, Green AA. Cellular DNA content as a predictor of response to chemotherapy in infants with unresectable neuroblastoma. N Engl J Med 1984; 311: 231–5. - PubMed
-
- Schwab M, Alitalo K, Klempnauer KH et al. Amplified DNA with limited homology to myc cellular oncogene is shared by human neuroblastoma cell lines and a neuroblastoma tumour. Nature 1983; 305: 245–8. - PubMed
-
- Brodeur GM, Seeger RC, Schwab M, Varmus HE, Bishop JM. Amplification of N‐myc in untreated human neuroblastomas correlates with advanced disease stage. Science 1984; 224: 1121–4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
