

Systematic review: Effects, design choices, and context of pay-for-performance in health care
- PMID: 20731816
- PMCID: PMC2936378
- DOI: 10.1186/1472-6963-10-247
Systematic review: Effects, design choices, and context of pay-for-performance in health care
Abstract
Background: Pay-for-performance (P4P) is one of the primary tools used to support healthcare delivery reform. Substantial heterogeneity exists in the development and implementation of P4P in health care and its effects. This paper summarizes evidence, obtained from studies published between January 1990 and July 2009, concerning P4P effects, as well as evidence on the impact of design choices and contextual mediators on these effects. Effect domains include clinical effectiveness, access and equity, coordination and continuity, patient-centeredness, and cost-effectiveness.
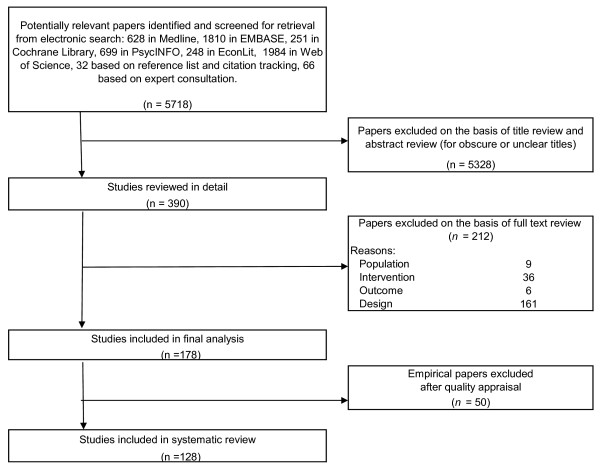
Methods: The systematic review made use of electronic database searching, reference screening, forward citation tracking and expert consultation. The following databases were searched: Cochrane Library, EconLit, Embase, Medline, PsychINFO, and Web of Science. Studies that evaluate P4P effects in primary care or acute hospital care medicine were included. Papers concerning other target groups or settings, having no empirical evaluation design or not complying with the P4P definition were excluded. According to study design nine validated quality appraisal tools and reporting statements were applied. Data were extracted and summarized into evidence tables independently by two reviewers.
Results: One hundred twenty-eight evaluation studies provide a large body of evidence -to be interpreted with caution- concerning the effects of P4P on clinical effectiveness and equity of care. However, less evidence on the impact on coordination, continuity, patient-centeredness and cost-effectiveness was found. P4P effects can be judged to be encouraging or disappointing, depending on the primary mission of the P4P program: supporting minimal quality standards and/or boosting quality improvement. Moreover, the effects of P4P interventions varied according to design choices and characteristics of the context in which it was introduced.Future P4P programs should (1) select and define P4P targets on the basis of baseline room for improvement, (2) make use of process and (intermediary) outcome indicators as target measures, (3) involve stakeholders and communicate information about the programs thoroughly and directly, (4) implement a uniform P4P design across payers, (5) focus on both quality improvement and achievement, and (6) distribute incentives to the individual and/or team level.
Conclusions: P4P programs result in the full spectrum of possible effects for specific targets, from absent or negligible to strongly beneficial. Based on the evidence the review has provided further indications on how effect findings are likely to relate to P4P design choices and context. The provided best practice hypotheses should be tested in future research.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
