

Nurse led interventions to improve control of blood pressure in people with hypertension: systematic review and meta-analysis
- PMID: 20732968
- PMCID: PMC2926309
- DOI: 10.1136/bmj.c3995
Nurse led interventions to improve control of blood pressure in people with hypertension: systematic review and meta-analysis
Abstract
Objective: To review trials of nurse led interventions for hypertension in primary care to clarify the evidence base, establish whether nurse prescribing is an important intervention, and identify areas requiring further study.
Design: Systematic review and meta-analysis.
Data sources: Ovid Medline, Cochrane Central Register of Controlled Trials, British Nursing Index, Cinahl, Embase, Database of Abstracts of Reviews of Effects, and the NHS Economic Evaluation Database.
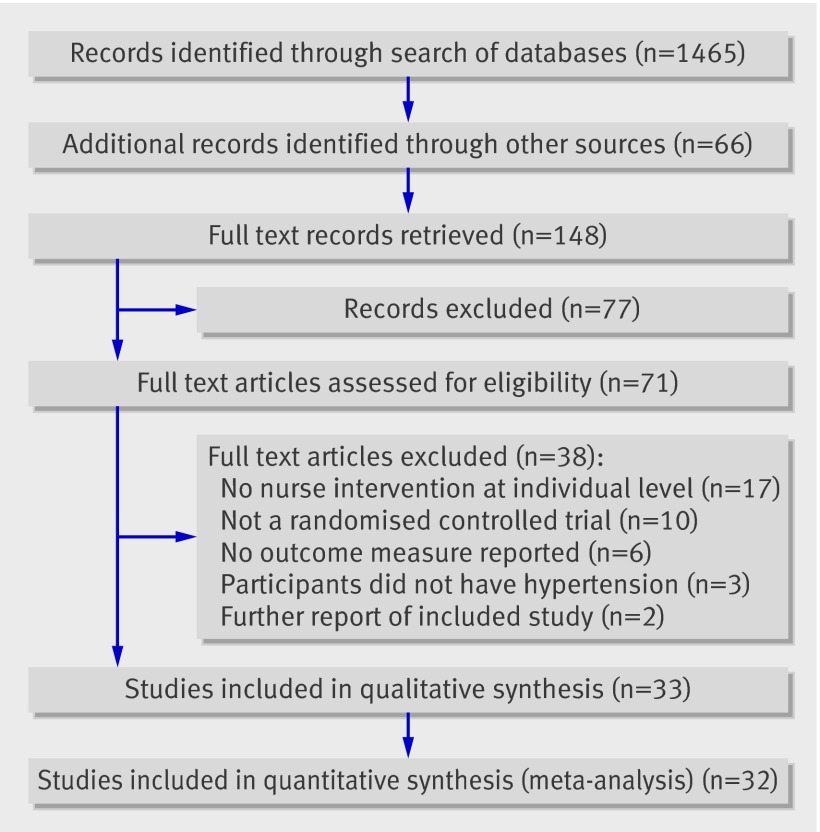
Study selection: Randomised controlled trials of nursing interventions for hypertension compared with usual care in adults.
Data extraction: Systolic and diastolic blood pressure, percentages reaching target blood pressure, and percentages taking antihypertensive drugs. Intervention effects were calculated as relative risks or weighted mean differences, as appropriate, and sensitivity analysis by study quality was undertaken.
Data synthesis: Compared with usual care, interventions that included a stepped treatment algorithm showed greater reductions in systolic blood pressure (weighted mean difference -8.2 mm Hg, 95% confidence interval -11.5 to -4.9), nurse prescribing showed greater reductions in blood pressure (systolic -8.9 mm Hg, -12.5 to -5.3 and diastolic -4.0 mm Hg, -5.3 to -2.7), telephone monitoring showed higher achievement of blood pressure targets (relative risk 1.24, 95% confidence interval 1.08 to 1.43), and community monitoring showed greater reductions in blood pressure (weighted mean difference, systolic -4.8 mm Hg, 95% confidence interval -7.0 to -2.7 and diastolic -3.5 mm Hg, -4.5 to -2.5).
Conclusions: Nurse led interventions for hypertension require an algorithm to structure care. Evidence was found of improved outcomes with nurse prescribers from non-UK healthcare settings. Good quality evidence from UK primary health care is insufficient to support widespread employment of nurses in the management of hypertension within such healthcare systems.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures






References
-
- Ezzati M, Lopez AD, Rodgers A, Vander Hoom S, Murray CJL, and the Comparative Risk Assessment Collaborating Group. Selected major risk factors and global and regional burden of disease. Lancet 2002;360:1347-60. - PubMed
-
- National Centre for Social Research. Health survey for England 2003. Department of Health, 2004.
-
- Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet 2005;365:217-23. - PubMed
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003;42:1206-52. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical