

A prospective cluster-randomized trial to implement the Canadian CT Head Rule in emergency departments
- PMID: 20732978
- PMCID: PMC2950184
- DOI: 10.1503/cmaj.091974
A prospective cluster-randomized trial to implement the Canadian CT Head Rule in emergency departments
Abstract
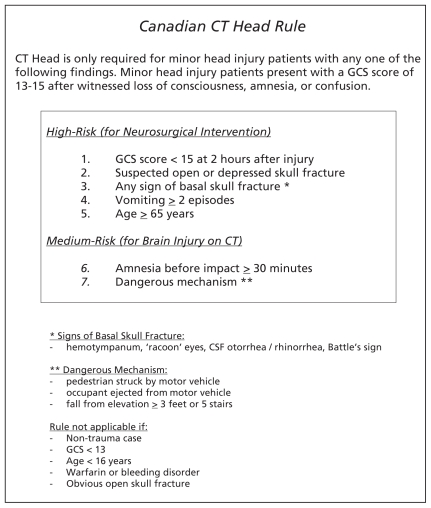
Background: The Canadian CT Head Rule was developed to allow physicians to be more selective when ordering computed tomography (CT) imaging for patients with minor head injury. We sought to evaluate the effectiveness of implementing this validated decision rule at multiple emergency departments.
Methods: We conducted a matched-pair cluster-randomized trial that compared the outcomes of 4531 patients with minor head injury during two 12-month periods (before and after) at hospital emergency departments in Canada, six of which were randomly allocated as intervention sites and six as control sites. At the intervention sites, active strategies, including education, changes to policy and real-time reminders on radiologic requisitions were used to implement the Canadian CT Head Rule. The main outcome measure was referral for CT scan of the head.
Results: Baseline characteristics of patients were similar when comparing control to intervention sites. At the intervention sites, the proportion of patients referred for CT imaging increased from the "before" period (62.8%) to the "after" period (76.2%) (difference +13.3%, 95% CI 9.7%-17.0%). At the control sites, the proportion of CT imaging usage also increased, from 67.5% to 74.1% (difference +6.7%, 95% CI 2.6%-10.8%). The change in mean imaging rates from the "before" period to the "after" period for intervention versus control hospitals was not significant (p = 0.16). There were no missed brain injuries or adverse outcomes.
Interpretation: Our knowledge-translation-based trial of the Canadian CT Head Rule did not reduce rates of CT imaging in Canadian emergency departments. Future studies should identify strategies to deal with barriers to implementation of this decision rule and explore more effective approaches to knowledge translation. (ClinicalTrials.gov trial register no. NCT00993252).
Figures
References
-
- Pitts SR, Niska RW, Xu J, et al. National Hospital Ambulatory Medical Care Survey: 2006 emergency department summary. Natl Health Stat Report. 2008 Aug 6;:1–38. - PubMed
-
- Seelig JM, Becker DP, Miller JD, et al. Traumatic acute subdural hematoma: major mortality reduction in comatose patients treated within four hours. N Engl J Med. 1981;304:1511–8. - PubMed
-
- Marshall LF, Toole BM, Bowers SA The National Traumatic Coma Data Bank. Part 2: Patients who talk and deteriorate: implications for treatment. J Neurosurg. 1983;59:285–8. - PubMed
-
- McCaig LF. National Hospital Ambulatory Medical Care Survey: 1992 emergency department summary. Adv Data. 1994;245:1–12. - PubMed
-
- Stiell IG, Wells GA, Vandemheen K, et al. Variation in ED use of computed tomography for patients with minor head injury. Ann Emerg Med. 1997;30:14–22. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical