

Referral pattern for epilepsy surgery after evidence-based recommendations: a retrospective study
- PMID: 20733145
- PMCID: PMC2931651
- DOI: 10.1212/WNL.0b013e3181eee457
Referral pattern for epilepsy surgery after evidence-based recommendations: a retrospective study
Erratum in
- Neurology. 2010 Nov 23;75(21):1945
Abstract
Background: Class I evidence for surgical effectiveness in refractory temporal lobe epilepsy (TLE) in 2001 led to an American Academy of Neurology practice parameter in 2003 recommending "referral to a surgical epilepsy center on failing appropriate trials of first-line antiepileptic drugs." We examined whether this led to a change in referral patterns to our epilepsy center.
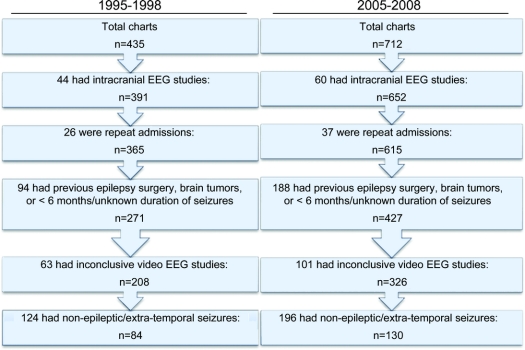
Methods: We compared referral data for patients with TLE at our center for 1995 to 1998 (group 1, n = 83) and 2005 to 2008 (group 2, n = 102) to determine whether these recommendations resulted in a change in referral patterns for surgical evaluation. Patients with brain tumors, previous epilepsy surgery evaluations, or brain surgery (including epilepsy surgery) were excluded.
Results: We did not find a difference between the groups in the duration from the diagnosis of habitual seizures to referral (17.1 +/- 10.0 vs 18.6 +/- 12.6 years, p = 0.39) or the age at the time of evaluation (34.1 +/- 10.3 vs 37.0 +/- 11.8 years, p = 0.08). However, there was a difference in the distributions of age at evaluation (p = 0.03) and the duration of pharmacotherapy (p = 0.03) between the groups, with a greater proportion of patients in group 2 with drug-resistant epilepsy both earlier and later in their treatment course. Nonepileptic seizures were referred significantly earlier than TLE in either group or when combined.
Conclusions: Our analysis does not identify a significantly earlier referral for epilepsy surgery evaluation as recommended in the practice parameter, but suggests a hopeful trend in this direction.
Figures


Comment in
-
Still an elusive target: guiding practice for epilepsy surgery.Neurology. 2010 Aug 24;75(8):678-9. doi: 10.1212/WNL.0b013e3181eee510. Neurology. 2010. PMID: 20733142 No abstract available.
Summary for patients in
-
Are epilepsy surgery guidelines being followed?Neurology. 2010 Aug 24;75(8):e41-2. doi: 10.1212/WNL.0b013e3181f1c031. Neurology. 2010. PMID: 20733140 No abstract available.
References
-
- Sander J. Some aspects of prognosis in the epilepsies: a review. Epilepsia 1993;34:1007–1016. - PubMed
-
- Kwan P, Brodie MJ. Early identification of refractory epilepsy. N Engl J Med 2000;342:314–319. - PubMed
-
- Wiebe S, Blume WT, Girvin JP, Eliasziw M. A randomized, controlled trial of surgery for temporal-lobe epilepsy. N Engl J Med 2001;345:311–318. - PubMed
-
- Engel J Jr, Wiebe S, French J, et al. Practice parameter: temporal lobe and localized neocortical resections for epilepsy—report of the Quality Standards Subcommittee of the American Academy of Neurology, in association with the American Epilepsy Society and the American Association of Neurological Surgeons. Neurology 2003;60:538–547. - PubMed
-
- Begley CE, Famulari M, Annegers JF, et al. The cost of epilepsy in the United States: an estimate from population-based clinical and survey data. Epilepsia 2000;41:342–351. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources