

Utility of early MRI in the diagnosis and management of acute spontaneous intracerebral hemorrhage
- PMID: 20733299
- PMCID: PMC2992640
- DOI: 10.1159/000316892
Utility of early MRI in the diagnosis and management of acute spontaneous intracerebral hemorrhage
Abstract
Background: The optimal diagnostic evaluation for spontaneous intracerebral hemorrhage (ICH) remains controversial. In this retrospective study, we assessed the utility of early magnetic resonance imaging (MRI) in ICH diagnosis and management.
Methods: Eighty-nine (72%) of 123 patients with spontaneous ICH underwent a brain CT and MRI within 30 days of ICH onset. Seventy patients with a mean age of 62 ± 15 years were included. A stroke neurologist and a general neurologist, each blinded to the final diagnosis, independently reviewed the admission data and the initial head CT and then assigned a presumed ICH cause under 1 of 9 categories. ICH cause was potentially modified after subsequent MRI review. The final 'gold standard' ICH etiology was determined after review of the complete medical record by an independent investigator. Change in diagnostic category and confidence and the potential impact on patient management were systematically recorded.
Results: Mean time to MRI was 3 ± 5 days. Final ICH diagnosis was hypertension or cerebral amyloid angiopathy (CAA) in 50% of patients. After MRI review the stroke neurologist changed diagnostic category in 14%, diagnostic confidence in an additional 23% and management in 20%, and the general neurologist did so in 19, 21 and 21% of patients, respectively. MRI yield was highest in ICH secondary to ischemic stroke, CAA, vascular malformations and neoplasms, and did not differ by age, history of hypertension, hematoma location or the presence of intraventricular hemorrhage.
Conclusions: The results of this study suggest potential additive clinical benefit of early MRI in patients with spontaneous ICH.
Copyright © 2010 S. Karger AG, Basel.
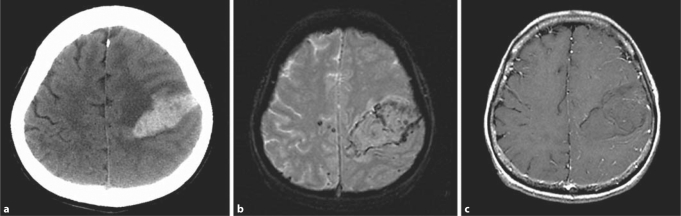
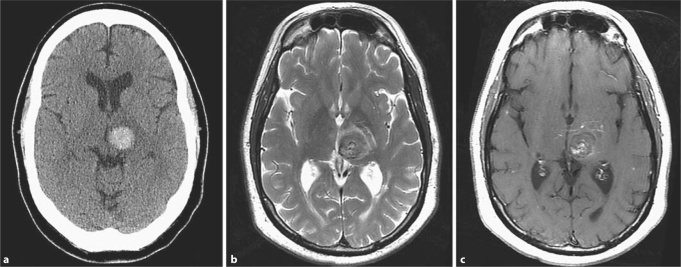
Figures
References
-
- Feigin VL, Lawes CM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol. 2009;8:355–369. - PubMed
-
- Brott T, Thalinger K, Hertzberg V. Hypertension as a risk factor for spontaneous intracerebral hemorrhage. Stroke. 1986;17:1078–1083. - PubMed
-
- Ohtani R, Kazui S, Tomimoto H, Minematsu K, Naritomi H. Clinical and radiographic features of lobar cerebral hemorrhage: hypertensive versus non-hypertensive cases. Intern Med. 2003;42:576–580. - PubMed
-
- Barnes B, Cawley CM, Barrow DL. ICH secondary to vascular lesions. Neurosurg Clin North Am. 2002;13:289–297. - PubMed
-
- McEvoy AW, Kitchen ND, Thomas DG. Intracerebral haemorrhage and drug abuse in young adults. Br J Neurosurg. 2000;14:449–454. - PubMed
