

A phase I dose-escalation study of oral BR-DIM (BioResponse 3,3'- Diindolylmethane) in castrate-resistant, non-metastatic prostate cancer
- PMID: 20733950
- PMCID: PMC2923864
A phase I dose-escalation study of oral BR-DIM (BioResponse 3,3'- Diindolylmethane) in castrate-resistant, non-metastatic prostate cancer
Abstract
3, 3'-diindolylmethane (DIM) modulates estrogen metabolism and acts as an anti-androgen which down-regulates the androgen receptor and prostate specific antigen (PSA). We conducted a dose-escalation, phase I study of BioResponse (BR)-DIM with objectives to determine the maximum tolerated dose (MTD), toxicity profile, and phar-macokinetics (PK) of BR-DIM, and to assess its effects on serum PSA and quality of life (QoL).
Patients and methods: Cohorts of 3-6 patients received escalating doses of twice daily oral BR-DIM providing DIM at 75 mg, then 150 mg, 225 mg, and 300 mg. Toxicity was evaluated monthly. Serum PSA and QoL were measured at baseline, monthly during treatment, and at end of study.
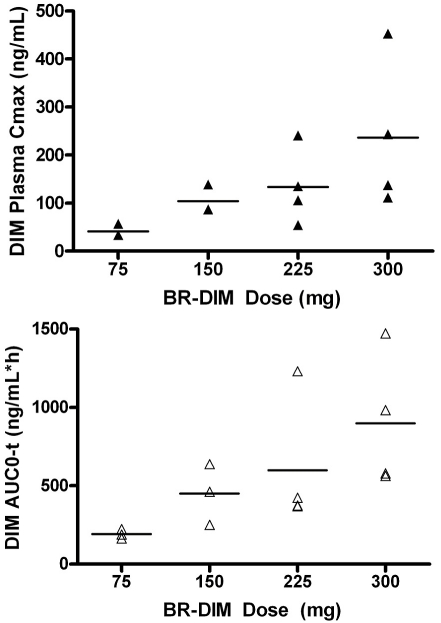
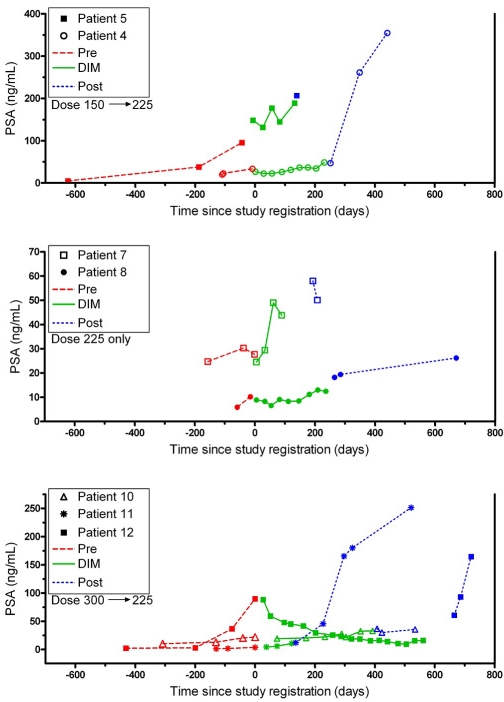
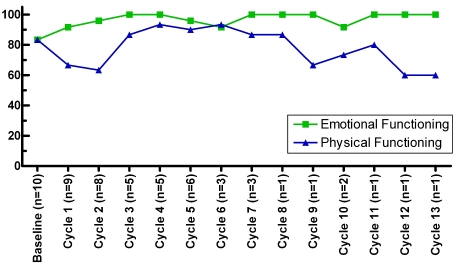
Results: 12 patients with castrate-resistant, non-metastatic, PSA relapse prostate cancer were treated over 4 dose cohorts; 2 patients (at 150 mg and 225 mg, respectively) underwent intra-patient dose escalation, by one dose level. After oral administration of the first dose of BR-DIM, the plasma exposure to DIM appeared dose proportional at doses ranging from 75 to 300 mg, with the mean C(max) and mean AUC(last) increasing from 41.6 to 236.4 ng/ml and from 192.0 to 899.0 ng/ml*h, respectively. Continued relatively stable systemic exposure to DIM was achieved following twice daily oral administration of BR-DIM. Minimal toxicity was observed. Two of the four patients treated at 300 mg had grade 3 asymptomatic hyponatremia (AH) discovered on routine blood work. The other 2 patients at this dose had no AH. Therefore, the maximum tolerated dose (MTD) was deemed to be 300 mgand the recommended phase II dose (RP2D) of BR-DIM was 225 mg twice daily. One patient without AH at 225 mg experienced a 50% PSA decline. One patient with BR-DIM dose of 225 mg had PSA stabilization. The other 10 patients had an initial deceleration of their PSA rise (decrease in slope), but eventually progressed based on continual PSA rise or evidence of metastatic disease. Ten patients completed monthly QoL reports for a mean of 6 months (range: 1-13). QoL measures emotional functioning may have held up somewhat better over time than their physical functioning.
Conclusion: BR-DIM was well tolerated. Increasing systemic exposure to DIM was achieved with the increase of BR-DIM dose. Modest efficacy was demonstrated. Patients' QoL varied over time with length of treatment. Phase II studies are recommended at the dose of 225 mg orally twice daily.
Keywords: BR-DIM; DIM; PSA relapse; clinical trial; diindolylmethane; indole-3-carbinol; phase I.
Figures
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–249. - PubMed
-
- Dillioglugil O, Leibman BD, Kattan MW, Seale-Hawkins C, Wheeler TM, Scardino PT. Hazard rates for progression after radical prostatectomy for clinically localized prostate cancer. Urology. 1997;50:93–99. - PubMed
-
- Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA. 1999;281:1591–1597. - PubMed
-
- Cannon GM, Jr, Walsh PC, Partin AW, Pound CR. Prostate-specific antigen doubling time in the identification of patients at risk for progression after treatment and biochemical recurrence for prostate cancer. Urology. 2003;62(Suppl 1):2–8. - PubMed
-
- Messing EM, Manola J, Sarosdy M, Wilding G, Crawford ED, Trump D. Immediate hormonal therapy compared with observation after radical prostatectomy and pelvic lymphadenectomy in men with node-positive prostate cancer. N Engl J Med. 1999;341:1781–1788. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous