

Clinical experience with a multifunctional, flexible surgery system for endolumenal, single-port, and NOTES procedures
- PMID: 20734085
- PMCID: PMC3032221
- DOI: 10.1007/s00464-010-1225-5
Clinical experience with a multifunctional, flexible surgery system for endolumenal, single-port, and NOTES procedures
Abstract
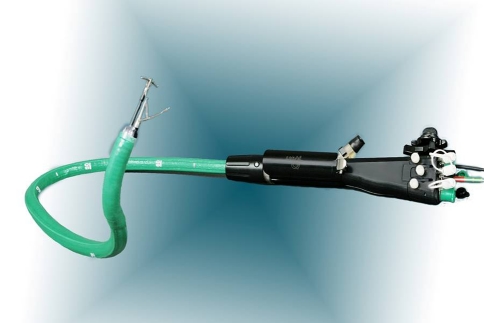
Background: Single-port and incisionless surgical approaches hold the promise of fewer complications, reduced pain, faster recovery, and improved cosmesis compared with traditional open or laparoscopic approaches. The ability to select an access approach (i.e., endolumenal, single-port, transvaginal, or transgastric) with one platform may be important to optimization of individual patient results. The authors report their results using these four separate surgical approaches tailored to three different therapeutic procedures, all with the use of a single flexible platform, the Incisionless Operating Platform (IOP).
Methods: After institutional review board approval, the IOP was used to perform nine cholecystectomies via transvaginal (TV) (n=4), transgastric (TG) (n=4), and single-port transumbilical (TU) (n=1) access. Two appendectomies were performed via TG access. Endolumenal access was used for 18 gastric pouch and stoma reductions after Roux-en-Y gastric bypass. The TG and TV procedures involved the use of one to three trocars. The recorded data included safety, procedural success, operative time, patient pain assessment (on a 0-10 scale) at discharge, and length of hospital stay.
Results: Procedural success was achieved for 16 of 18 endolumenal procedures, 1 of 1 single-port procedure, and 10 of 10 NOTES procedures. For 5 of 10 NOTES procedures, only one small trocar was required. The mean operative times were 79 min for pouch with stoma reduction, 171 min for cholecystectomy, and 274 min for appendectomy. Of 29 patients, 27 were discharged in 24 h or less. The average pain scores were 0.44 for pouch with stoma reduction, 1.3 for cholecystectomy, and 2.5 for appendectomy. No significant complications occurred. The ergonomics of IOP allowed the surgeon to interface with the system using an endoscopic or laparoscopic orientation.
Conclusion: Availability of a multifunctional, flexible surgery platform provides a choice of a single-port or incisionless surgical approach with the potential to reduce complications, pain, and recovery time while improving cosmesis.
Figures


References
-
- Keus F, deJong JA, Gooszen HG, vanLaarhoven CJ (2006) Laparoscopic versus open cholecystectomy for patients with symptomatic cholelithiasis. Cochrane Database Syst Rev 4:CD006231 - PubMed
-
- Pasricha P, Kozarek R, Swain P, Swanstrom LL, Raju G, Gross S, Saadat V, Rothe C, Birkett D (2005) Development of a next-generation therapeutic endoscope. Gastrointest Endosc 61:AB106–AB108
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
