

Periprocedural myocardial infarction: review and classification
- PMID: 20734444
- PMCID: PMC6653301
- DOI: 10.1002/clc.20819
Periprocedural myocardial infarction: review and classification
Abstract
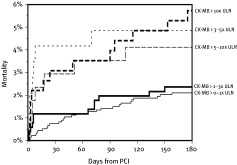
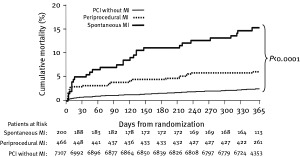
Technical and pharmacologic advances have reduced the occurrence of large periprocedural myocardial infarction (PMI) after percutaneous coronary interventions (PCI), but PMI still occurs in 6% to 18% of the cases and is associated with impaired short- and long-term survival. PMI might be due to side branch closure or flow-limiting dissection, but is most often diagnosed after apparently uncomplicated PCI and is due to atheroembolization into the microcirculation. Various definitions of PMI are used in clinical trials, but a rise in creatine kinase-MB greater than 3 to 8 times the upper limit of normal is consistently associated with worse prognosis, particularly as it reflects a more extensive and unstable atherosclerotic burden. On the other hand, data regarding the independent prognostic value of periprocedural troponin increase are conflicting. Some data suggest that PMI has a better prognosis than a spontaneously occurring myocardial infarction, and that its incidence is reduced with aggressive antiplatelet and statin therapy.
Figures
References
-
- Alpert JS, Thygesen K, Antman E, et al. Myocardial infarction redefined—a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol 2000;36:959–969. - PubMed
-
- Thygesen K, Alpert JS, White HD; Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction. Universal Definition of Myocardial Infarction. ESC/ACCF/AHA/WHF Expert Consensus Document. J Am Coll Cardiol 2007;50:2173–2195. - PubMed
-
- Stone GW, McLaurin BT, Cox DA, et al. Bivalirudin for patients with acute coronary syndromes. N Engl J Med 2006;355:2203–2216. - PubMed
-
- Giugliano RP, White JA, Boden C, et al. Early versus delayed, provisional eptifibatide in acute coronary syndromes. N Engl J Med 2009;360:2176–2190. - PubMed
-
- Mehta SR, Granger CB, Boden WE, et al. Early versus delayed invasive intervention in acute coronary syndromes. N Engl J Med 2009;360:2165–2175. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
