

Review
doi: 10.1016/j.mcna.2010.06.001.
The patient with sore throat
Affiliations
- PMID: 20736104
- PMCID: PMC7094485
- DOI: 10.1016/j.mcna.2010.06.001
Item in Clipboard
Review
The patient with sore throat
Med Clin North Am.
2010 Sep.
Abstract
Sore throat is a common medical complaint seen by the emergency practitioner, internist, pediatrician, and otolaryngologist. The differential for sore throat is vast. However, with a directed history this can often be narrowed down to 2 to 3 possible diagnoses. By paying particular attention to the associated symptoms and duration of symptoms, common self-limited etiologies like viral pharyngitis and nonstreptococcal tonsillitis can be distinguished from those that require more investigation, such as supraglottitis and tonsillar cancer. A sore throat is most commonly caused by an infectious, inflammatory, or neoplastic etiologic factor.
Copyright 2010 Elsevier Inc. All rights reserved.
Figures
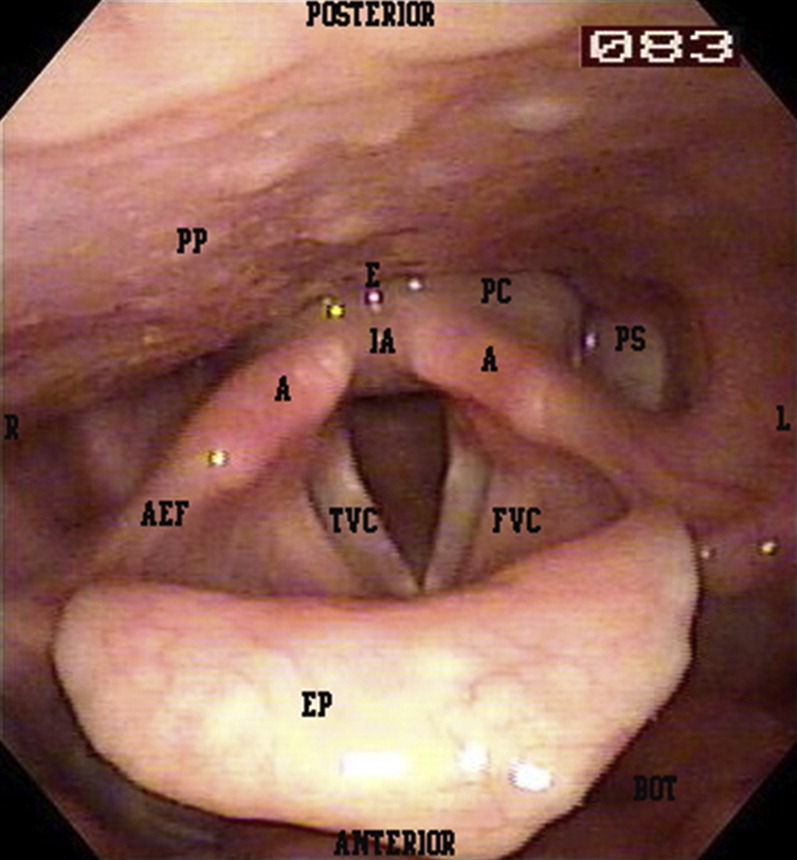
Fiberoptic view of laryngeal anatomy. A, arytenoid; BOT, base of tongue; E, esophageal inlet; EP, epiglottis; FVC, false vocal cord; IA, interarytenoid mucosa; PC, postcricoid mucosa; PP, posterior pharyngeal wall; PS, pyriform sinus; TVC, true vocal cord.
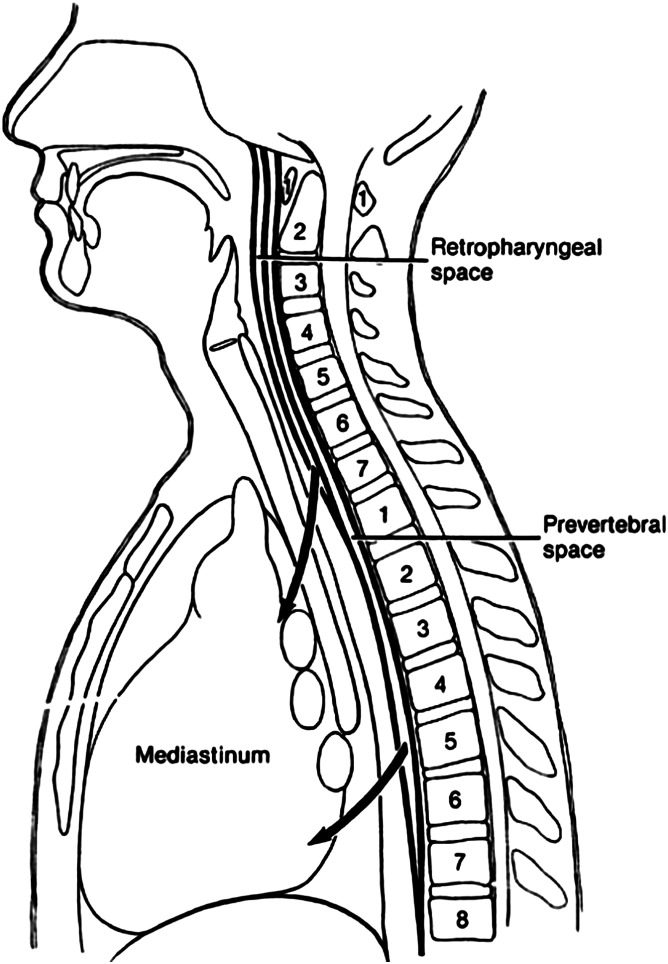
Retropharyngeal and prevertebral spaces and their relationship to the spinal column and mediastinum.
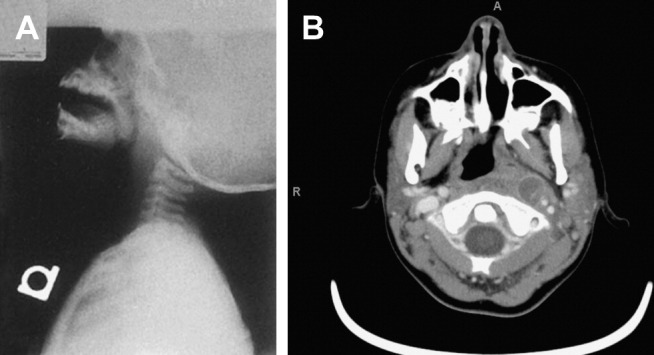
Retropharyngeal abscess. (A) lateral neck radiograph shows widening of the soft tissues anterior to the vertebral bodies. (From Flint PW. Cummings otolaryngology: head & neck surgery, 5th edition. St. Louis (MO): Mosby Elsevier; 2010. Chapter 196, Fig. 196-7A and B; with permission.) (B) CT scan with contrast of neck shows rim-enhancing collection consistent with a left retropharyngeal abscess.
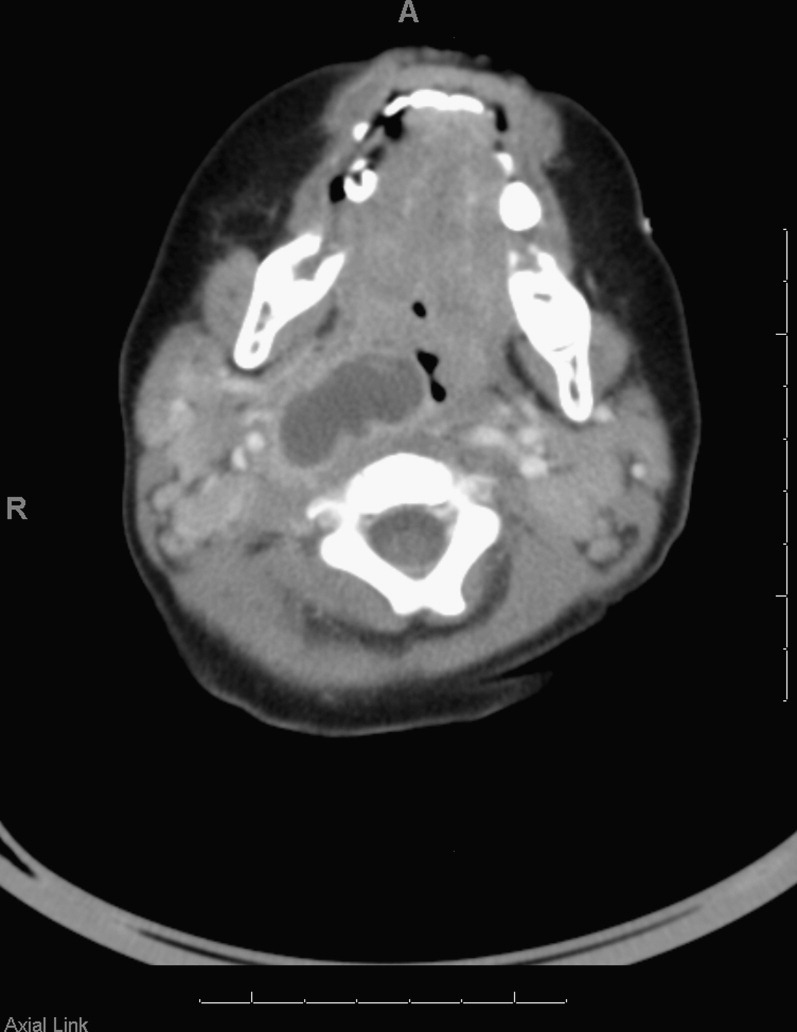
Right parapharyngeal abscess with impingement on the airway.

Epiglottitis. Widened epiglottis (asterisk) and aryepiglottic folds (arrowheads).

Laryngeal changes from chronic reflux. Edema of the interarytenoid mucosa (asterisk). Irregular, edematous, and erythematous true vocal cord mucosa (arrowheads).
Similar articles
-
The sore throat. Pharyngitis and epiglottitis.Infect Dis Clin North Am. 1988 Mar;2(1):149-62. Infect Dis Clin North Am. 1988. PMID: 3074105 Review.
-
Evaluation on immediate analgesic efficacy and safety of Kai-Hou-Jian spray (children's type) in treating sore throat caused by acute pharyngitis and tonsillitis in children: study protocol for a randomized controlled trial.Trials. 2021 Mar 18;22(1):216. doi: 10.1186/s13063-021-05148-1. Trials. 2021. PMID: 33736674 Free PMC article.
-
A Lot to Choke on: Case of Adult Epiglottitis with Concurrent Peritonsillar Abscess in a Patient with a Sore Throat.J Emerg Med. 2018 Dec;55(6):841-844. doi: 10.1016/j.jemermed.2018.09.017. Epub 2018 Oct 17. J Emerg Med. 2018. PMID: 30342860
-
Sore throat in primary care project: a clinical score to diagnose viral sore throat.Fam Pract. 2015 Jun;32(3):263-8. doi: 10.1093/fampra/cmv015. Epub 2015 Mar 25. Fam Pract. 2015. PMID: 25808403 Free PMC article.
-
An approach to diagnosing the acute sore throat.Am Fam Physician. 1997 Jan;55(1):131-8, 141-2. Am Fam Physician. 1997. PMID: 9012273 Review.
Cited by
-
Efficacy of a benzocaine lozenge in the treatment of uncomplicated sore throat.Eur Arch Otorhinolaryngol. 2012 Feb;269(2):571-7. doi: 10.1007/s00405-011-1802-9. Epub 2011 Oct 21. Eur Arch Otorhinolaryngol. 2012. PMID: 22015737 Clinical Trial.
-
Suspected Gastroparesis With Concurrent Gastroesophageal Reflux Disease Induced by Low-Dose Liraglutide.Cureus. 2022 Jul 16;14(7):e26916. doi: 10.7759/cureus.26916. eCollection 2022 Jul. Cureus. 2022. PMID: 35983392 Free PMC article.
-
Head-and-neck Cancer in the Emergency Department: A Contemporary Review of Common Presentations and Management.J Emerg Trauma Shock. 2024 Jan-Mar;17(1):33-39. doi: 10.4103/jets.jets_40_23. Epub 2024 Feb 28. J Emerg Trauma Shock. 2024. PMID: 38681881 Free PMC article. Review.
-
Evaluating the Efficacy of a Multidisciplinary Approach to Chronic Pharyngitis Treatment: A Retrospective Cohort Analysis.Cureus. 2025 Mar 18;17(3):e80772. doi: 10.7759/cureus.80772. eCollection 2025 Mar. Cureus. 2025. PMID: 40248524 Free PMC article.
-
Soothing Properties of Glycerol in Cough Syrups for Acute Cough Due to Common Cold.Pharmacy (Basel). 2017 Jan 20;5(1):4. doi: 10.3390/pharmacy5010004. Pharmacy (Basel). 2017. PMID: 28970416 Free PMC article. Review.
References
-
- Schappert S.M., Burt C.W. Ambulatory care visits to physician offices, hospital outpatient departments, and emergency departments: United States, 2001-02. Vital Health Stat 13. 2006;159:1–66. - PubMed
-
- Ayanruoh S., Waseem M., Quee F. Impact of rapid streptococcal test on antibiotic use in a pediatric emergency department. Pediatr Emerg Care. 2009;25(11):748–750. - PubMed
-
- Finkelstein Y., Bar-Ziv J., Nachmani A. Peritonsillar abscess as a cause of transient velopharyngeal insufficiency. Cleft Palate Craniofac J. 1993;30(4):421–428. - PubMed
-
- Bisno A. Acute pharyngitis. N Engl J Med. 2001;344(3):205–211. - PubMed
-
- Hoagland R.J. Infectious mononucleosis. Prim Care. 1975;2:295–307. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
