

Tumour necrosis is a postoperative prognostic marker for pancreatic cancer patients with a high interobserver reproducibility in histological evaluation
- PMID: 20736942
- PMCID: PMC2965866
- DOI: 10.1038/sj.bjc.6605854
Tumour necrosis is a postoperative prognostic marker for pancreatic cancer patients with a high interobserver reproducibility in histological evaluation
Abstract
Background: Tumour necrosis reflects the presence of hypoxia, which can be indicative of an aggressive tumour phenotype. The aim of this study was to investigate whether histological necrosis is a useful predictor of outcome in patients with pancreatic ductal carcinoma (PDC).
Methods: We reviewed histopathological findings in 348 cases of PDC in comparison with clinicopathological information. We counted small necrotic foci (micronecrosis) as necrosis, in addition to massive necrosis that had been only defined as necrosis in previous studies. The reproducibility of identifying histological parameters was tested by asking five independent observers to blindly review 51 examples of PDC.
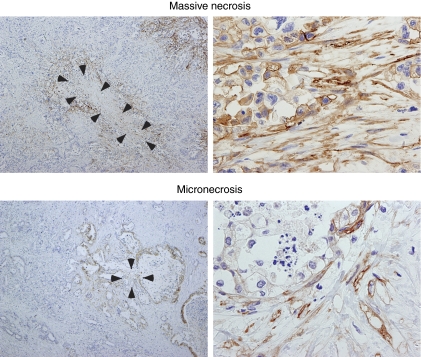
Results: Both micronecrosis and massive necrosis corresponded to hypoxic foci expressing carbonic anhydrase IX detected by immunohistochemistry. Multivariate survival analysis showed that histological necrosis was an independent predictor of poor outcome in terms of both disease-free survival (DFS) and disease-specific survival (DSS) of PDC patients. In addition, metastatic status, and lymphatic, venous, and intrapancreatic neural invasion were independent prognostic factors for shorter DFS and metastatic status, margin status, lymphatic invasion, and intrapancreatic neural invasion were independent prognostic factors for DSS. The interobserver reproducibility of necrosis identification among the five independent observers was 'almost perfect' (κ-value of 0.87).
Conclusion: Histological necrosis is a simple, accurate, and reproducible predictor of postoperative outcome in PDC patients.
Figures



References
-
- Adsay NV, Basturk O, Bonnett M, Kilinc N, Andea AA, Feng J, Che M, Aulicino MR, Levi E, Cheng JD (2005) A proposal for a new and more practical grading scheme for pancreatic ductal adenocarcinoma. Am J Surg Pathol 29: 724–733 - PubMed
-
- Bristow RG, Hill RP (2008) Hypoxia and metabolism. Hypoxia, DNA repair and genetic instability. Nat Rev Cancer 8: 180–192 - PubMed
-
- Center for Cancer Control and Information Services, National Cancer Center Japan (2009) Cancer Statistics in Japan
-
- Chia SK, Wykoff CC, Watson PH, Han C, Leek RD, Pastorek J, Gatter KC, Ratcliffe P, Harris AL (2001) Prognostic significance of a novel hypoxia-regulated marker, carbonic anhydrase IX, in invasive breast carcinoma. J Clin Oncol 19: 3660–3668 - PubMed
-
- Couvelard A, O’Toole D, Leek R, Turley H, Sauvanet A, Degott C, Ruszniewski P, Belghiti J, Harris AL, Gatter K, Pezzella F (2005) Expression of hypoxia-inducible factors is correlated with the presence of a fibrotic focus and angiogenesis in pancreatic ductal adenocarcinomas. Histopathology 46: 668–676 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
