

Dyslipidemia in children with chronic kidney disease
- PMID: 20736985
- PMCID: PMC3222564
- DOI: 10.1038/ki.2010.311
Dyslipidemia in children with chronic kidney disease
Abstract
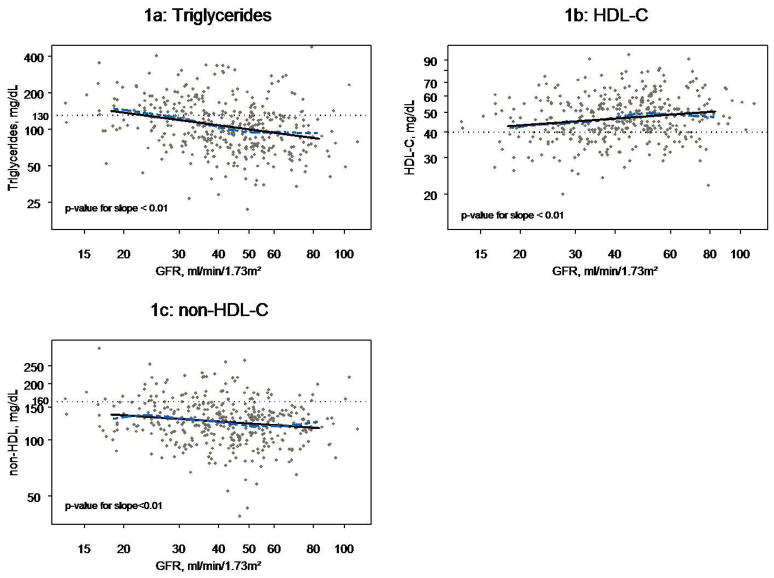
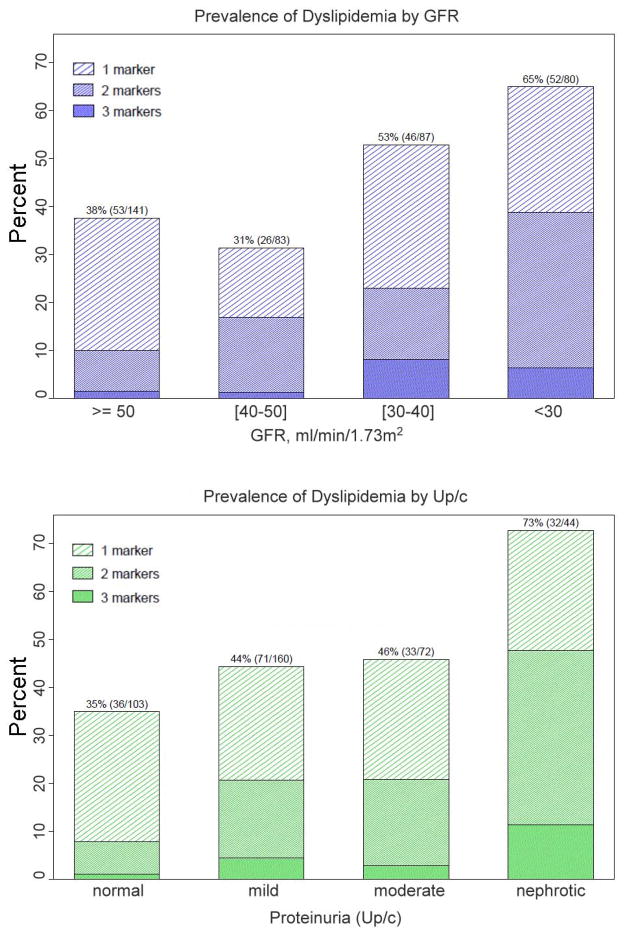
Dyslipidemia, a known risk factor for atherosclerosis, is frequent among both adults and children with chronic kidney disease. Here, we describe the prevalence and pattern of dyslipidemia from a cross-sectional analysis of 391 children aged 1-16 years, enrolled in the multicenter Chronic Kidney Disease in Children (CKiD) study, with a median glomerular filtration rate (GFR), measured by the plasma disappearance of iohexol, of 43 ml/min per 1.73 m2. Multivariate analysis was applied to adjust for age, gender, body mass index (BMI), GFR, and the urinary protein/creatinine ratio. Proteinuria was in the nephrotic range in 44 and the BMI exceeded the 95th percentile in 57 patients of this cohort. Baseline lipid analysis found a high prevalence of hypertriglyceridemia in 126, increased non-HDL-C in 62, and reduced HDL-C in 83. Overall, 177 children had dyslipidemia, of whom 79 had combined dyslipidemia. Lower GFR was associated with higher triglycerides, lower HDL-C, and higher non-HDL-C. Nephrotic-range proteinuria was significantly associated with dyslipidemia and combined dyslipidemia. Compared with children with a GFR>50, children with a GFR<30 had significantly increased odds ratios for any dyslipidemia or for combined dyslipidemia. Hence, among children with moderate chronic kidney disease, dyslipidemia is common and is associated with lower GFR, nephrotic proteinuria, and non-renal factors including age and obesity.
Conflict of interest statement
Disclosure:
None of the authors’ have relationships with companies that may have a financial interest in the information contained in the manuscript.
Figures
References
-
- Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998;32:S112–S119. - PubMed
-
- K/DOQI clinical practice guidelines for management of dyslipidemias in patients with kidney disease. Am J Kidney Dis. 2003;41:I–IV. S1–91. - PubMed
-
- Saland JM, Ginsberg HN. Lipoprotein metabolism in chronic renal insufficiency. Pediatr Nephrol. 2007;22:1095–1112. - PubMed
-
- Fried LF, Orchard TJ, Kasiske BL. Effect of lipid reduction on the progression of renal disease: a meta-analysis. Kidney Int. 2001;59:260–269. - PubMed
-
- Saito T, Oikawa S, Sato H, Sasaki J. Lipoprotein glomerulopathy: renal lipidosis induced by novel apolipoprotein E variants. Nephron. 1999;83:193–201. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
