

The quality of emergency medical care in baden-württemberg (Germany): four years in focus
- PMID: 20737058
- PMCID: PMC2925343
- DOI: 10.3238/arztebl.2010.0523
The quality of emergency medical care in baden-württemberg (Germany): four years in focus
Abstract
Background: In 2004, the German federal state of Baden-Württemberg implemented a quality management system for pre-hospital emergency care. Since then, there has been a semi-annual assessment of the frequency of different types of emergency medical interventions and the quality of care.
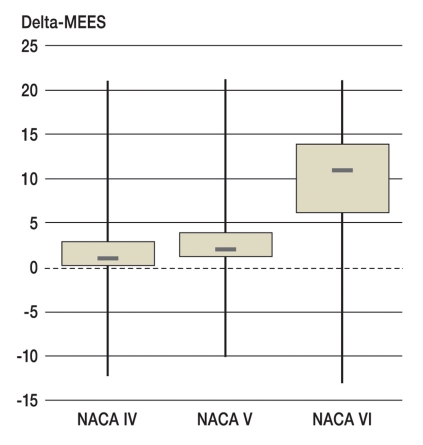
Methods: The frequencies of different types of intervention were determined and reported both in absolute numbers and as incidence figures, i.e., interventions per 1000 inhabitants per year. The quality of care was rated with the Mainz Emergency Evaluation Score (MEES), and analyses of resuscitation outcomes and guideline implementation were performed.
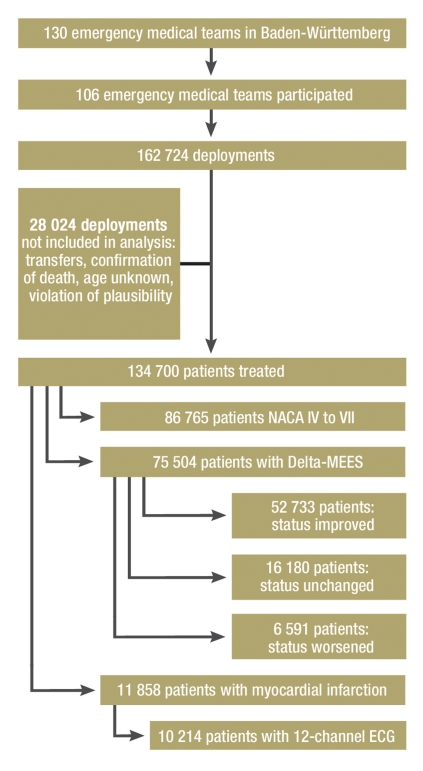
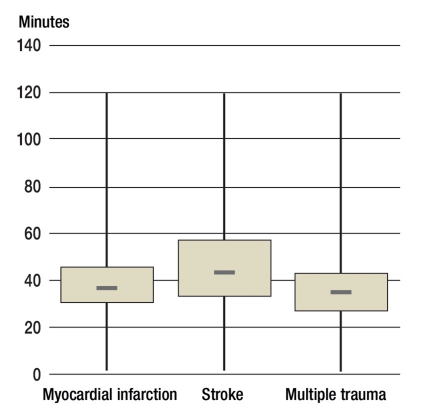
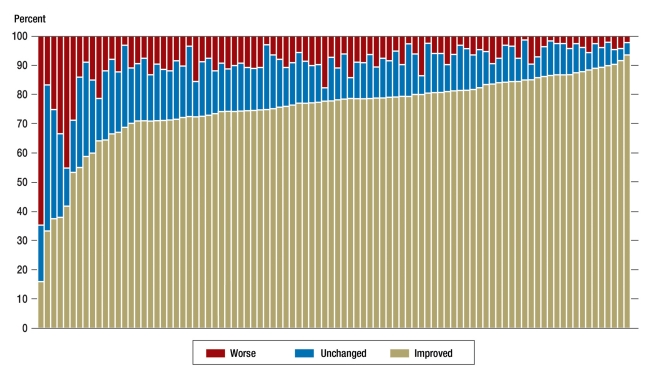
Results: From 2004 to 2008, there were a total of 524,833 pre-hospital emergency medical interventions in Baden-Württemberg. The annual incidence of emergency interventions rose by 22% over this period (from 16.2 to 19.9 interventions per 1000 inhabitants per year), and the percentage of patients who were severely ill or severely injured rose as well, from 47.3% to 51.1%. The percentage of patients over age 75 rose from 29.1% to 31.3%. 11,858 patients with myocardial infarction (MI) were treated in 2008; the incidence of treatment for MI rose by 60% from 2004 to 2008, from 0.907 to 1.448 interventions per 1000 inhabitants per year. A major improvement in the diagnostic evaluation of MI came about through the purchase of more 12-channel ECG machines. In 2008, the emergency medical teams succeeded in improving the patient's condition in 69.07% of all cases (77.9% for MI, 63.2% for stroke, 74.4% for multiple trauma). 21 patients per 100,000 inhabitants per year arrived in the hospital alive after out-of-hospital cardiac arrest and pre-hospital resuscitation.
Conclusions: Even in the face of increasing utilization, the quality of emergency medical care in Baden-Württemberg has remained high. Since a quality management system was introduced in 2004, the physicians in charge of emergency medical teams have had access to the data that they need in order to evaluate and further develop the services that they provide.
Figures
Comment in
-
Analyses are indispensable.Dtsch Arztebl Int. 2011 Feb;108(6):94; author reply 95. doi: 10.3238/arztebl.2011.0094a. Epub 2011 Feb 11. Dtsch Arztebl Int. 2011. PMID: 21373276 Free PMC article. No abstract available.
-
Delta-MEES is not very practical.Dtsch Arztebl Int. 2011 Feb;108(6):94-5; author reply 95. doi: 10.3238/arztebl.2011.0094b. Epub 2011 Feb 11. Dtsch Arztebl Int. 2011. PMID: 21373277 Free PMC article. No abstract available.
-
Far from reality.Dtsch Arztebl Int. 2011 Feb;108(6):95; author reply 95. doi: 10.3238/arztebl.2011.0095a. Epub 2011 Feb 11. Dtsch Arztebl Int. 2011. PMID: 21373278 Free PMC article. No abstract available.
References
-
- Messelken M, et al. Externe Qualitätssicherung im Rettungsdienst. Notfall & Rettungsmedizin. 2005;8:476–483.
-
- Messelken M, Schlechtriemen T. Der minimale Notarztdatensatz MIND2. Notfall & Rettungsmedizin. 2003;6:189–192.
-
- Messelken M, Dirks B. Zentrale Auswertung von Notarzteinsätzen im Rahmen externer Qualitätssicherung. Notfall & Rettungsmedizin. 2001;4:408–415.
-
- Hennes HJ, Reinhardt T, Dick W. Beurteilung des Notfallpatienten mit dem Mainz Emergency Evaluation Score MEES. Notfallmedizin. 1992;18:130–136.
-
- Tryba M, Brüggemann H, Echtermeyer V. Klassifizerung von Erkrankungen und Verletzungen in Notarztrettungssystemen. Notfallmedizin. 1980;6:725–727.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical