

Prognostic factors and long-term outcomes of childhood nasopharyngeal carcinoma
- PMID: 20737561
- PMCID: PMC2994981
- DOI: 10.1002/cncr.25376
Prognostic factors and long-term outcomes of childhood nasopharyngeal carcinoma
Abstract
Background: The authors studied the survival and long-term morbidities of children with nasopharyngeal carcinoma (NPC).
Methods: This was a retrospective review of children with NPC who were treated at St. Jude Children's Research Hospital between 1961 and 2004. Prognostic factors and long term effects of therapy were analyzed.
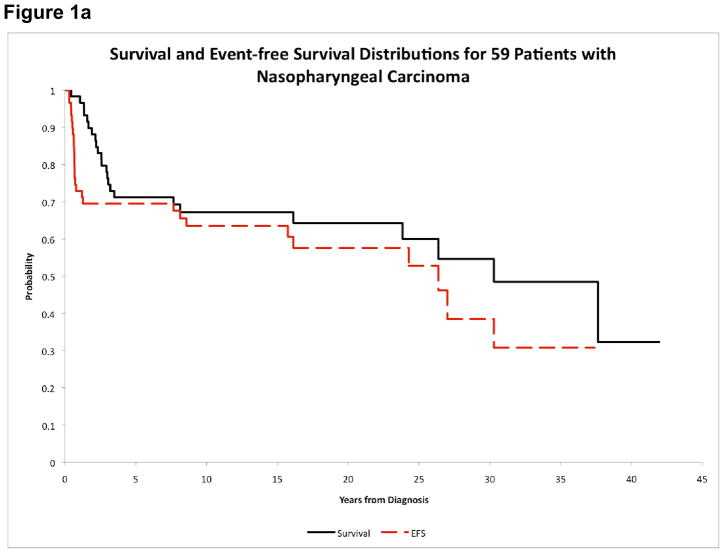
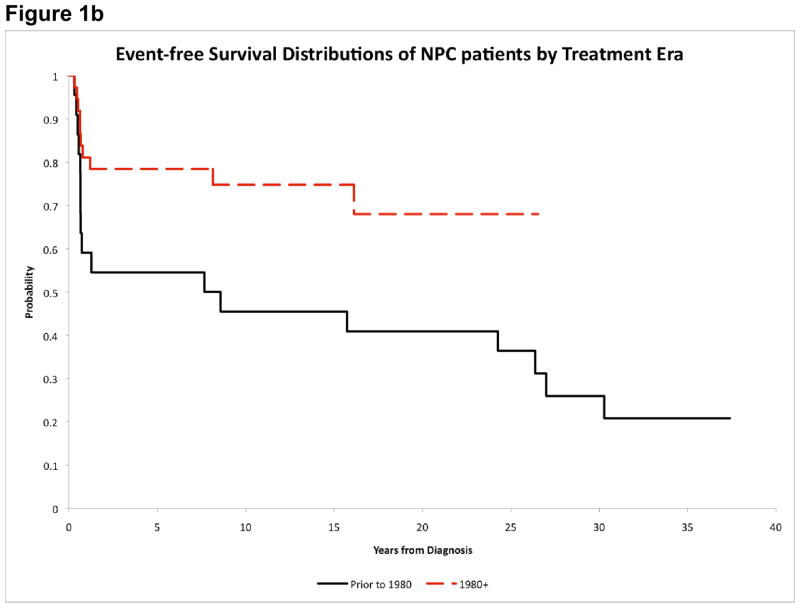
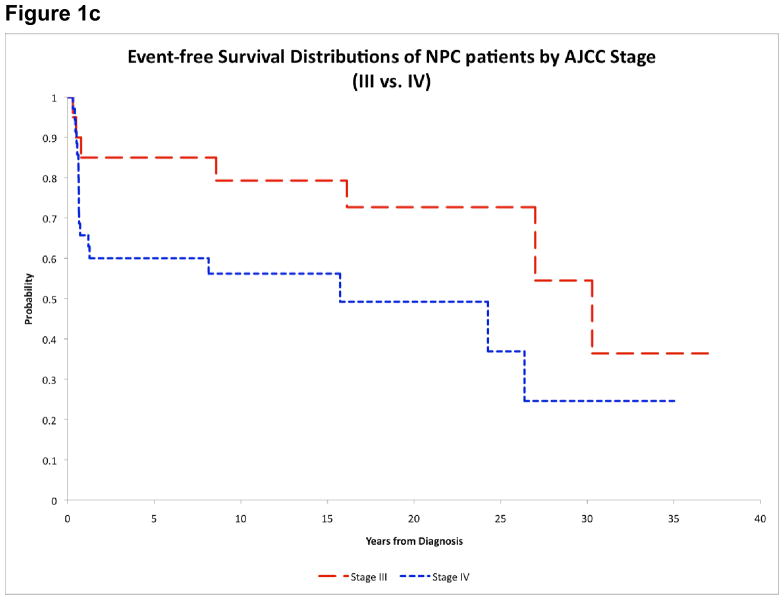
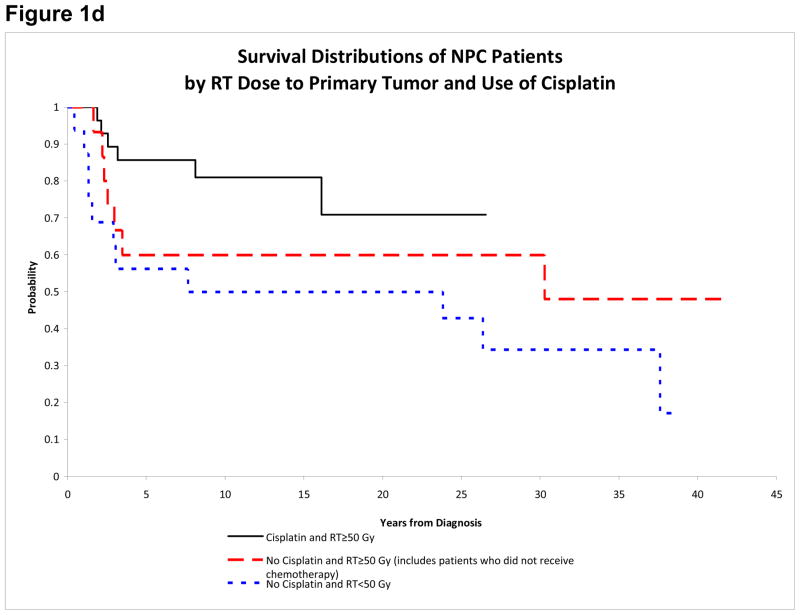
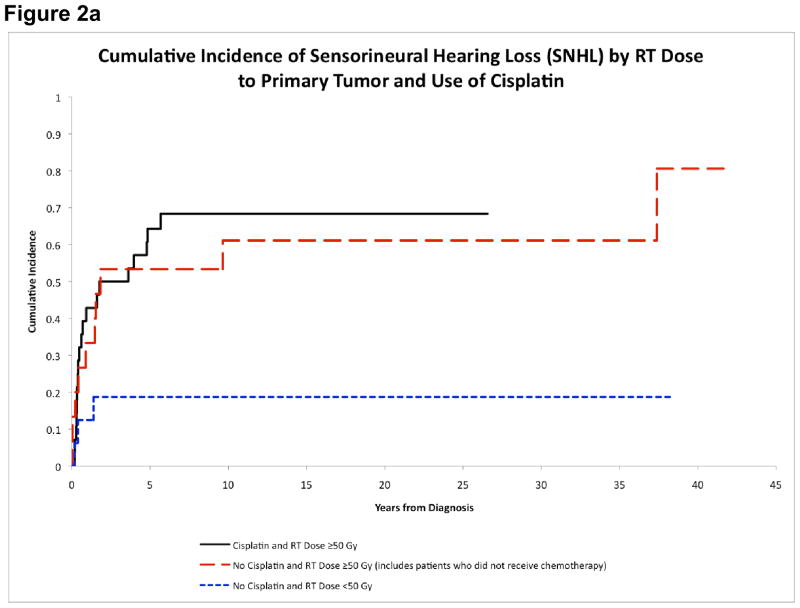
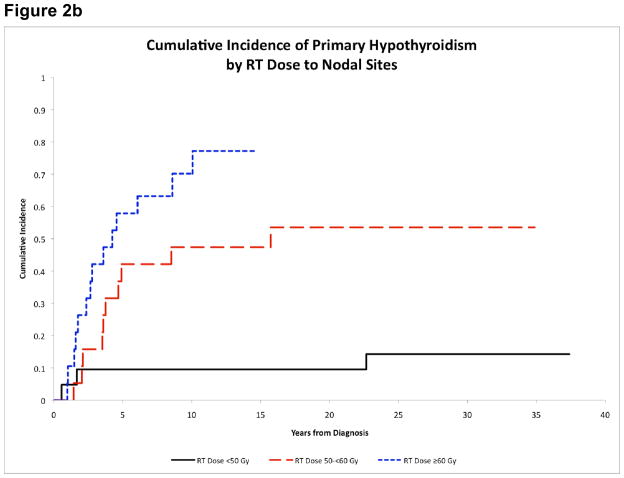
Results: Fifty-nine patients (median age, 14.1 years) were identified. Most were male (66.1%) and black (54.2%) and had lymphoepithelioma (93.2%). Thirty-five patients had stage IV disease (59.3%), 20 patients had stage III disease (33.9%), and 4 patients had stage II disease (6.8%). All patients received radiotherapy (RT) to the primary tumor, and most received cervical RT (98.3%) and chemotherapy (88.1%). The 15-year survival and event-free survival (EFS) rates were 67.2% ± 7.5% and 63.5% ± 7.8%, respectively. Five patients (8.5%) developed subsequent malignancies 8.6 to 27 years after NPC diagnosis. EFS was improved in patients who were diagnosed after 1980 (74.8% ± 10% vs 45.5% ± 10.1%; P = .031), in patients who had stage III disease compared with patients who had stage IV disease (79.3% ± 9.6% vs 56.2% ± 11.8%; P = .049), in patients who received cisplatin (81% ± 10.7% vs 45.8% ± 9.7%; P = .013), and in patients who received ≥ 50 grays of RT (71.4% ± 9.3% vs 43.8% ± 11.6%; P = .048). White patients had higher distant failure rates than black patients (41.7% ± 10.4% vs 15.6 ± 6.5%; P = .045). The 15-year cumulative incidence (CI) of any morbidity was 83.7% ± 5.4%, the CI of sensorineural hearing loss was 52.9% ± 6.7%, the CI of primary hypothyroidism was 42.7% ± 6.6%, and the CI of growth hormone deficiency (GHD) was 14.1% ± 4.7%. Dose-response relations were observed between the RT dose and primary hypothyroidism and GHD.
Conclusions: The outcome of children with NPC improved over the past 4 decades with the use of cisplatin-based chemotherapy and higher RT doses. However, many survivors had long-term treatment-related morbidities.
© 2010 American Cancer Society.
Figures
References
-
- Ayan I, Altun M. Nasopharyngeal carcinoma in children: retrospective review of 50 patients. Int J Radiat Oncol Biol Phys. 1996;35(3):485–92. - PubMed
-
- Ayan I, Kaytan E, Ayan N. Childhood nasopharyngeal carcinoma: from biology to treatment. Lancet Oncol. 2003;4(1):13–21. - PubMed
-
- Vokes EE, Liebowitz DN, Weichselbaum RR. Nasopharyngeal carcinoma. Lancet. 1997;350(9084):1087–91. - PubMed
-
- Langendijk JA, Leemans CR, Buter J, Berkhof J, Slotman BJ. The additional value of chemotherapy to radiotherapy in locally advanced nasopharyngeal carcinoma: a meta-analysis of the published literature. J Clin Oncol. 2004;22(22):4604–12. - PubMed
-
- Pao WJ, Hustu HO, Douglass EC, Beckford NS, Kun LE. Pediatric nasopharyngeal carcinoma: long term follow-up of 29 patients. Int J Radiat Oncol Biol Phys. 1989;17(2):299–305. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
