

Spinal schistosomiasis: differential diagnosis for acute paraparesis in a U.S. resident
- PMID: 20737799
- PMCID: PMC2920119
- DOI: 10.1080/10790268.2010.11689703
Spinal schistosomiasis: differential diagnosis for acute paraparesis in a U.S. resident
Abstract
Background: Spinal schistosomiasis is a severe presentation of Schistosoma mansoni infection, which is endemic in South America, the Middle East, and sub-Saharan Africa. With increasing international travel, a disease can spread from an endemic area to another part of the world easily.
Objectives: To present a case of a US resident who developed acute paraparesis due to spinal schistosomiasis after traveling to sub-Saharan Africa.
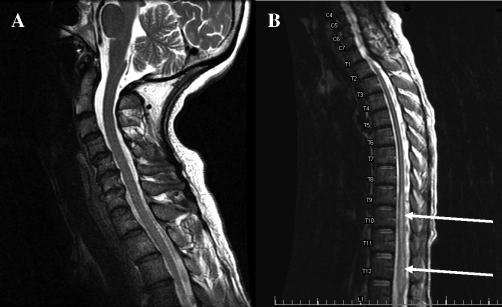
Participant: A 45-year-old woman presented with abdominal pain radiating into the bilateral lower extremities. She was diagnosed with a pelvic mass and underwent an urgent hysterectomy with right salpingo-oopherectomy. Postoperatively, she developed progressive weakness with worsening pain in her bilateral lower extremities and neurogenic bladder. Magnetic resonance imaging showed an abnormal T2 hyperintense signal in the entire spinal cord below the T3 level with abnormal contrast enhancement from T9 through the conus medullaris. Spinal fluid analysis showed lymphocytic pleocytosis and elevated protein. The patient was diagnosed with transverse myelitis. Subsequently, a detailed history revealed a visit to Ethiopia 2 years earlier. Tests for S mansoni were positive. After treatment with praziquantel and prednisone, her neurologic function began to improve.
Conclusions: An increasing incidence of international travel is increasing the likelihood of US physicians' encountering this treatable condition. Travelers with spinal schistosomiasis may not have symptoms of systemic infection. Therefore, it is important to include spinal schistosomiasis in the differential diagnosis of acute inflammatory myelopathy, particularly with a history of travel to endemic areas.
Figures


References
-
- Prevention and Control of Schistosomiasis and Soil-Transmitted Helminthiasis: Report of a WHO Expert Committee. 2002. World Health Organization, Geneva, Technical Report Series No. 912; - PubMed
-
- Ross AG, Bartley PB, Sleigh AC, et al. Schistosomiasis. N Engl J Med. 2002;346(16):1212–1220. - PubMed
-
- Carod-Artal FJ. Neurological complications of Schistosoma infection. Trans R Soc Trop Med Hyg. 2008;102(2):107–116. - PubMed
-
- Ferrari TC. Involvement of central nervous system in the schistosomiasis. Mem Inst Oswaldo Cruz. 2004;99(suppl I):59–62. - PubMed
-
- Hancock K, Tsang V. Development and optimization of the FAST-ELISA for detecting antibodies to Schistosoma mansoni. J Immunol Methods. 1986;92(2):167–176. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources