

Neurologic disease burden in treated HIV/AIDS predicts survival: a population-based study
- PMID: 20739646
- PMCID: PMC3013488
- DOI: 10.1212/WNL.0b013e3181f4d5bb
Neurologic disease burden in treated HIV/AIDS predicts survival: a population-based study
Abstract
Background: Combination antiretroviral therapy (cART) has improved the survival of patients with HIV/AIDS but its impact remains uncertain on the changing prevalence and incidence of neurologic disorders with ensuing effects on mortality.
Methods: The prevalence and incidence of neurologic disorders were examined in patients receiving active care in a regional HIV care program from 1998 to 2008. The mortality hazard ratio (HR) was calculated by Cox proportional hazard models with adjustment for demographic and clinical variables.
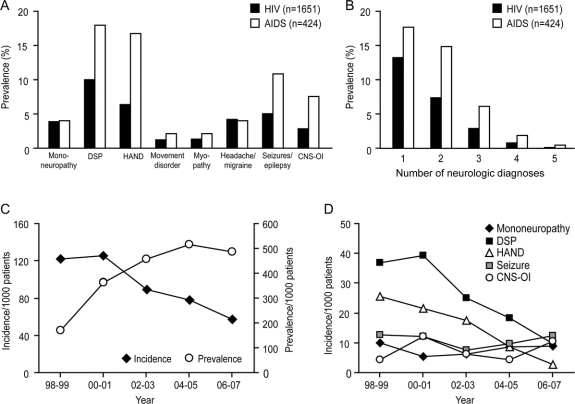
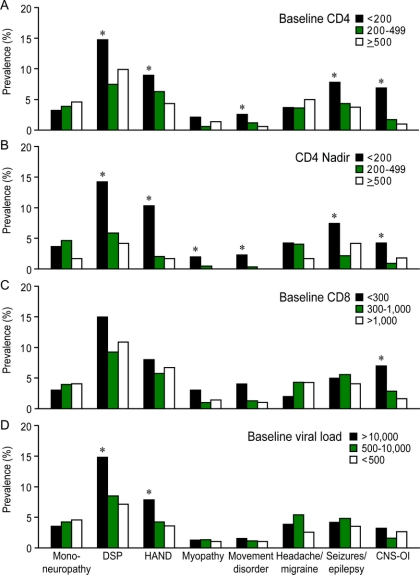
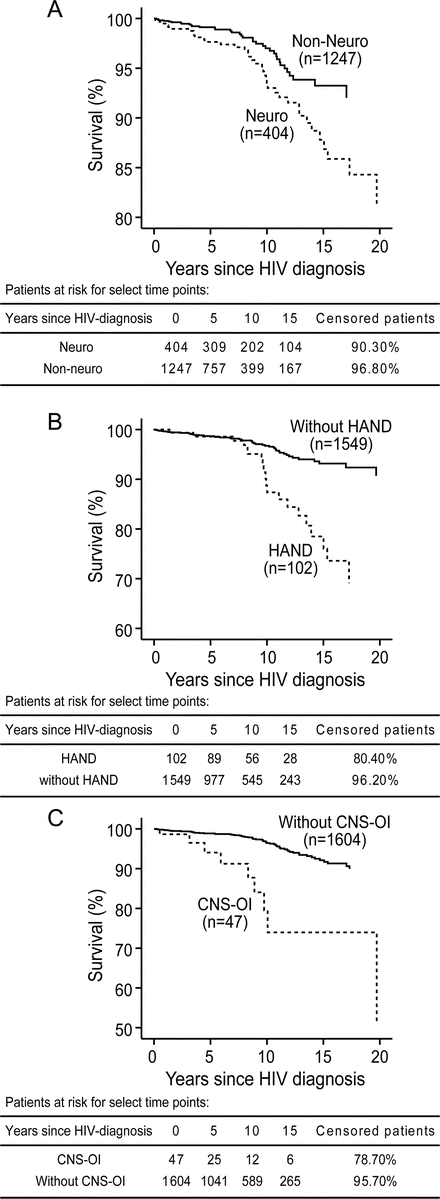
Results: Of 1,651 HIV-infected patients assessed, 404 (24.5%) were identified as having one or more neurologic disorders, while 41% of AIDS-affected persons exhibited neurologic disease. Symptomatic distal sensory polyneuropathy (DSP, 10.0%) and HIV-associated neurocognitive disorder (HAND, 6.2%) represented the most prevalent disorders among 53 recognized neurologic disorders. Patients with at least one neurologic disorder exhibited higher mortality rates (17.6% vs 8.0%, p < 0.0001), particularly AIDS-related deaths (9.7% vs 3.2%, p < 0.0001), compared with those without neurologic disorders. The highest mortality HR was associated with opportunistic infections of CNS (HR 5.3, 95% confidence interval [CI] 2.5-11.2), followed by HAND (HR 3.1, 95% CI 1.8-5.3) and the presence of any neurologic disorder (HR 2.0, 95% CI 1.2-3.2). The risk of AIDS-related death with a neurologic disorder was increased by 13.3% per 100 cells/mm(3) decrement in blood CD4+ T-cell levels or by 39% per 10-fold increment in plasma viral load.
Conclusions: The burden and type of HIV-related neurologic disease have evolved over the past decade and despite the availability of cART, neurologic disorders occur frequently and predict an increased risk of death.
Figures



References
-
- Mocroft A, Ledergerber B, Katlama C, et al. Decline in the AIDS and death rates in the EuroSIDA study: an observational study. Lancet 2003;362:22–29. - PubMed
-
- Authier FJ, Chariot P, Gherardi RK. Skeletal muscle involvement in human immunodeficiency virus (HIV)-infected patients in the era of highly active antiretroviral therapy (HAART). Muscle Nerve 2005;32:247–260. - PubMed
-
- Sacktor N. The epidemiology of human immunodeficiency virus-associated neurological disease in the era of highly active antiretroviral therapy. J Neurovirol 2002;8(suppl 2):115–121. - PubMed
-
- McArthur JC, Haughey N, Gartner S, et al. Human immunodeficiency virus-associated dementia: an evolving disease. J Neurovirol 2003;9:205–221. - PubMed
-
- Dore GJ, McDonald A, Li Y, Kaldor JM, Brew BJ. Marked improvement in survival following AIDS dementia complex in the era of highly active antiretroviral therapy. AIDS 2003;17:1539–1545. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous