

Activation of voltage-gated KCNQ/Kv7 channels by anticonvulsant retigabine attenuates mechanical allodynia of inflammatory temporomandibular joint in rats
- PMID: 20796319
- PMCID: PMC2936374
- DOI: 10.1186/1744-8069-6-49
Activation of voltage-gated KCNQ/Kv7 channels by anticonvulsant retigabine attenuates mechanical allodynia of inflammatory temporomandibular joint in rats
Abstract
Background: Temporomandibular disorders (TMDs) are characterized by persistent orofacial pain and have diverse etiologic factors that are not well understood. It is thought that central sensitization leads to neuronal hyperexcitability and contributes to hyperalgesia and spontaneous pain. Nonsteroidal anti-inflammatory drugs (NSAIDs) are currently the first choice of drug to relieve TMD pain. NSAIDS were shown to exhibit anticonvulsant properties and suppress cortical neuron activities by enhancing neuronal voltage-gated potassium KCNQ/Kv7 channels (M-current), suggesting that specific activation of M-current might be beneficial for TMD pain.
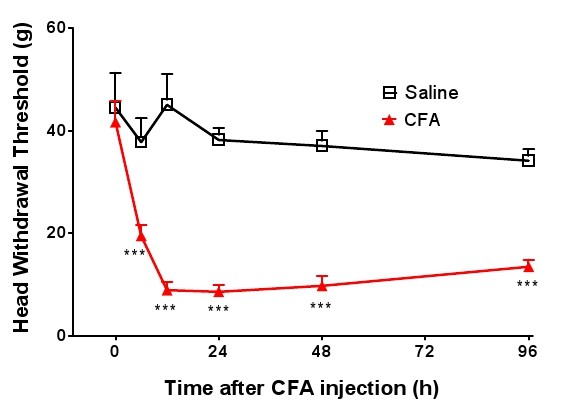
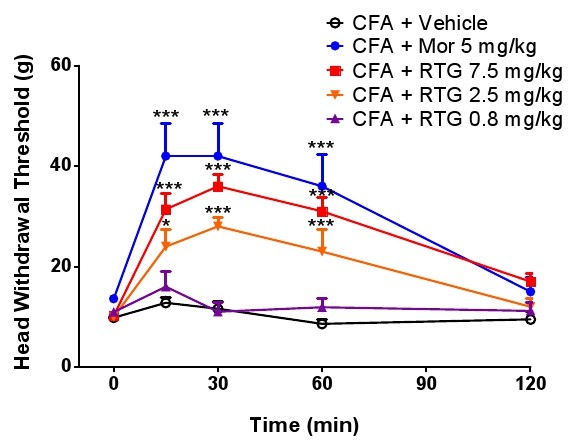
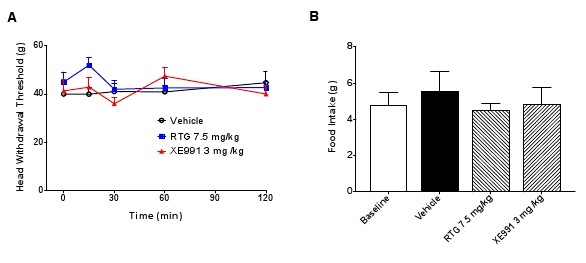
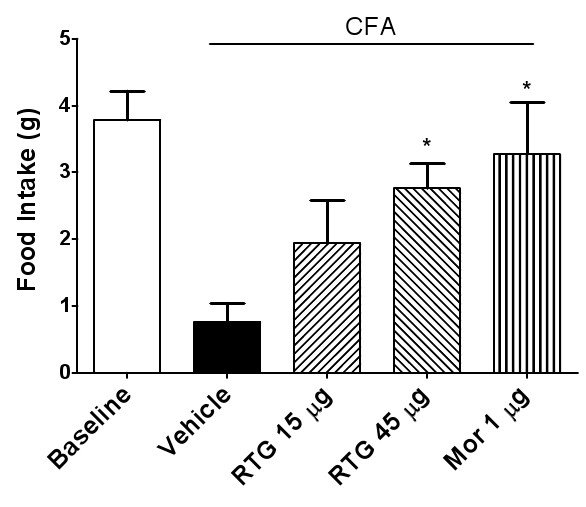
Results: In this study, we selected a new anticonvulsant drug retigabine that specifically activates M-current, and investigated the effect of retigabine on inflammation of the temporomandibular joint (TMJ) induced by complete Freund's adjuvant (CFA) in rats. The results show that the head withdrawal threshold for escape from mechanical stimulation applied to facial skin over the TMJ in inflamed rats was significantly lower than that in control rats. Administration of centrally acting M-channel opener retigabine (2.5 and 7.5 mg/kg) can dose-dependently raise the head withdrawal threshold of mechanical allodynia, and this analgesic effect can be reversed by the specific KCNQ channel blocker XE991 (3 mg/kg). Food intake is known to be negatively associated with TMJ inflammation. Food intake was increased significantly by the administration of retigabine (2.5 and 7.5 mg/kg), and this effect was reversed by XE991 (3 mg/kg). Furthermore, intracerebralventricular injection of retigabine further confirmed the analgesic effect of central retigabine on inflammatory TMJ.
Conclusions: Our findings indicate that central sensitization is involved in inflammatory TMJ pain and pharmacological intervention for controlling central hyperexcitability by activation of neuronal KCNQ/M-channels may have therapeutic potential for TMDs.
Figures





Similar articles
-
Activation of peripheral KCNQ channels attenuates inflammatory pain.Mol Pain. 2014 Feb 21;10:15. doi: 10.1186/1744-8069-10-15. Mol Pain. 2014. PMID: 24555569 Free PMC article.
-
Suppression of KCNQ/M (Kv7) potassium channels in the spinal cord contributes to the sensitization of dorsal horn WDR neurons and pain hypersensitivity in a rat model of bone cancer pain.Oncol Rep. 2015 Mar;33(3):1540-50. doi: 10.3892/or.2015.3718. Epub 2015 Jan 14. Oncol Rep. 2015. PMID: 25592230
-
The anti-hyperalgesic activity of retigabine is mediated by KCNQ potassium channel activation.Naunyn Schmiedebergs Arch Pharmacol. 2004 Apr;369(4):382-90. doi: 10.1007/s00210-004-0881-1. Epub 2004 Mar 9. Naunyn Schmiedebergs Arch Pharmacol. 2004. PMID: 15007538
-
Retigabine: chemical synthesis to clinical application.CNS Drug Rev. 2005 Spring;11(1):1-20. doi: 10.1111/j.1527-3458.2005.tb00033.x. CNS Drug Rev. 2005. PMID: 15867950 Free PMC article. Review.
-
The mechanism of action of retigabine (ezogabine), a first-in-class K+ channel opener for the treatment of epilepsy.Epilepsia. 2012 Mar;53(3):412-24. doi: 10.1111/j.1528-1167.2011.03365.x. Epub 2012 Jan 5. Epilepsia. 2012. PMID: 22220513 Review.
Cited by
-
Nociceptive behavioural assessments in mouse models of temporomandibular joint disorders.Int J Oral Sci. 2020 Sep 29;12(1):26. doi: 10.1038/s41368-020-00095-0. Int J Oral Sci. 2020. PMID: 32989215 Free PMC article.
-
Pharmacological Activation of Neuronal Voltage-Gated Kv7/KCNQ/M-Channels for Potential Therapy of Epilepsy and Pain.Handb Exp Pharmacol. 2021;267:231-251. doi: 10.1007/164_2021_458. Handb Exp Pharmacol. 2021. PMID: 33837465
-
Behavioral and neuro-functional consequences of eliminating the KCNQ3 GABA binding site in mice.Front Mol Neurosci. 2023 May 25;16:1192628. doi: 10.3389/fnmol.2023.1192628. eCollection 2023. Front Mol Neurosci. 2023. PMID: 37305551 Free PMC article.
-
TET1 Participates in Complete Freund's Adjuvant-induced Trigeminal Inflammatory Pain by Regulating Kv7.2 in a Mouse Model.Neurosci Bull. 2024 Jun;40(6):707-718. doi: 10.1007/s12264-023-01139-1. Epub 2023 Nov 16. Neurosci Bull. 2024. PMID: 37973721 Free PMC article.
-
Activation of peripheral KCNQ channels relieves gout pain.Pain. 2015 Jun;156(6):1025-1035. doi: 10.1097/j.pain.0000000000000122. Pain. 2015. PMID: 25735002 Free PMC article.
References
-
- Brazeau GA. et al.The role of pharmacy in the management of patients with temporomandibular disorders and orofacial pain. J Am Pharm Assoc (Wash) 1998;38(3):354–61. quiz 362-3. - PubMed
-
- Sarlani E. et al.Evidence for up-regulated central nociceptive processing in patients with masticatory myofascial pain. J Orofac Pain. 2004;18(1):41–55. - PubMed
-
- Denucci DJ, Dionne RA, Dubner R. Identifying a neurobiologic basis for drug therapy in TMDs. J Am Dent Assoc. 1996;127(5):581–93. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
