

Evidence that the acute phase of ischemic preconditioning does not require signaling by the A 2B adenosine receptor
- PMID: 20797398
- PMCID: PMC2958103
- DOI: 10.1016/j.yjmcc.2010.08.015
Evidence that the acute phase of ischemic preconditioning does not require signaling by the A 2B adenosine receptor
Abstract
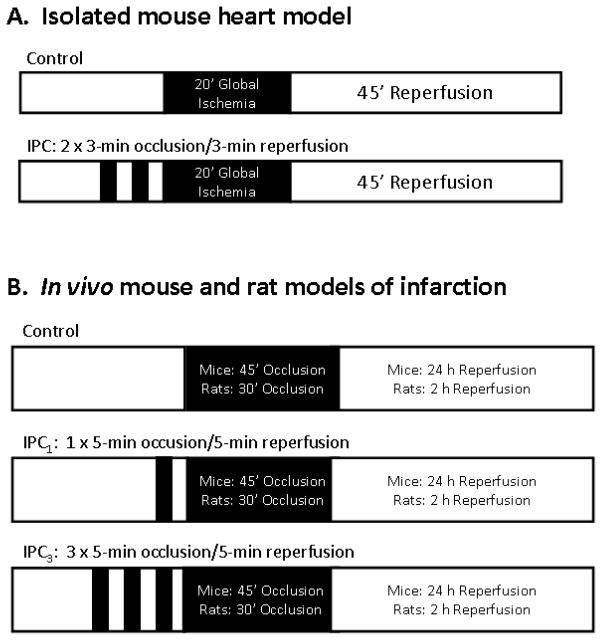
Ischemic preconditioning (IPC) is a protective phenomenon in which brief ischemia renders the myocardium resistant to subsequent ischemic insults. Here, we used A(2B)AR gene knock-out (A(2B)KO)/β-galactosidase reporter gene knock-in mice and the A(2B)AR antagonist ATL-801 to investigate the potential involvement of the A(2B)AR in IPC, focusing on the acute phase of protection. Cardioprotection provided by acute IPC elicited by two 3-min occlusion/3-min reperfusion cycles was readily apparent in an isolated, Langendorff-perfused mouse heart model in studies using hearts from A(2B)KO mice. IPC equivalently improved the recovery of contractile function following 20 min of global ischemia and 45 min of reperfusion in both WT and A(2B)KO hearts by ~30-40%, and equivalently decreased the release of cardiac troponin I during the reperfusion period (from 5969 ± 925 to 1595 ± 674 ng/g and 4376 ± 739 to 2278 ± 462 ng/g using WT and A(2B)KO hearts, respectively). Similarly, the infarct size-reducing capacity of acute IPC in an in vivo model of infarction was fully manifested in experiments using A(2B)KO mice, as well as in experiments using rats pretreated with ATL-801. We did observe, however, a marked reduction in infarct size in rats following administration of the selective A(2B)AR agonist BAY 60-6583 (~25% reduction at a dose of 1.0mg/kg). While supportive of its concept as a cardioprotective receptor, these experiments indicate that the mechanism of the early phase of IPC is not dependent on signaling by the A(2B)AR. We present the idea that the A(2B)AR may contribute to the later stages of IPC dependent on the induction of stress-responsive genes.
Copyright © 2010 Elsevier Ltd. All rights reserved.
Figures




References
-
- Murry CE, Jennings RB, Reimer KA. Preconditioning with ischemia: a delay of lethal cell injury in ischemic myocardium. Circulation. 1986:1124–36. - PubMed
-
- Miura T, Goto M, Urabe K, Endoh A, Shimamoto K, Iimura O. Does myocardial stunning contribute to infarct size limitation by ischemic preconditioning? Circulation. 1991;84:2504–12. - PubMed
-
- Murry CE, Richard VJ, Jennings RB, Reimer KA. Myocardial protection is lost before contractile function recovers from ischemic preconditioning. Am J Physiol. 1991;260:H796–804. - PubMed
-
- Van Winkle DM, Thornton JD, Downey DM, Downey JM. The natural history of preconditioning: cardioprotection depends on the duration of transient ischemia and time to subsequent ischemia. Cor Art Dis. 1991;2:613–9.
-
- Bolli R. The late phase of preconditioning. Circ Res. 2000;87:972–83. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
