

The interplay of socioeconomic status, distance to center, and interdonor service area travel on kidney transplant access and outcomes
- PMID: 20798250
- PMCID: PMC2994090
- DOI: 10.2215/CJN.04940610
The interplay of socioeconomic status, distance to center, and interdonor service area travel on kidney transplant access and outcomes
Abstract
Background and objectives: Variation in kidney transplant access across the United States may motivate relocation of patients with ability to travel to better-supplied areas.
Design, setting, participants, & measurements: We examined national transplant registry and U.S. Census data for kidney transplant candidates listed in 1999 to 2009 with a reported residential zip code (n = 203,267). Cox's regression was used to assess associations of socioeconomic status (SES), distance from residence to transplant center, and relocation to a different donation service area (DSA) with transplant access and outcomes.
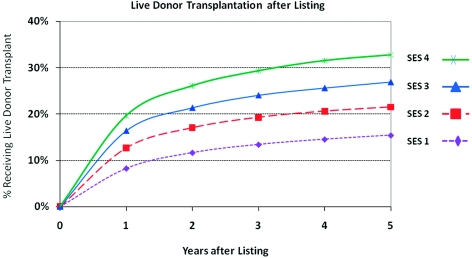
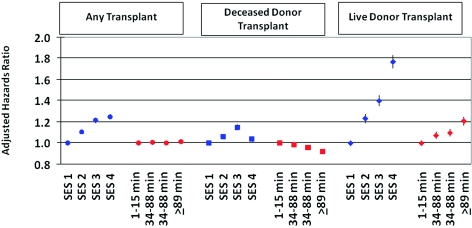
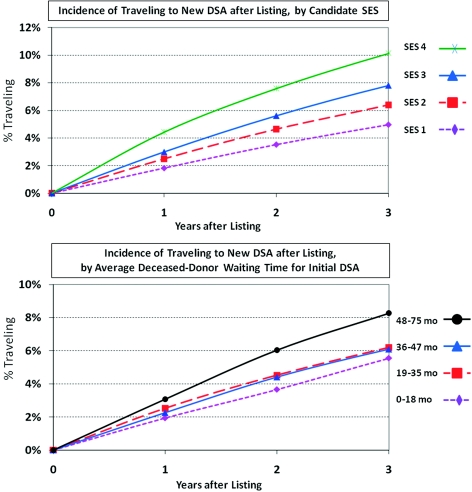
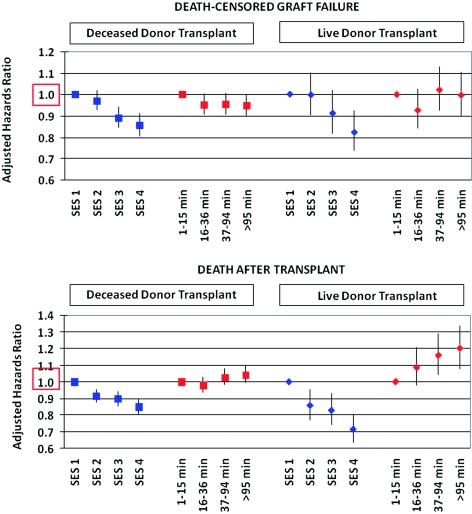
Results: Patients in the highest SES quartile had increased access to transplant compared with those with lowest SES, driven strongly by 76% higher likelihood of living donor transplantation (adjusted hazard ratio [aHR] 1.76, 95% confidence interval [CI] 1.70 to 1.83). Waitlist death was reduced in high compared with low SES candidates (aHR 0.86, 95% CI 0.84 to 0.89). High SES patients also experienced lower mortality after living and deceased donor transplant. Patients living farther from the transplant center had reduced access to deceased donor transplant and increased risk of post-transplant death. Inter-DSA travel was associated with a dramatic increase in deceased donor transplant access (HR 1.94, 95% CI 1.88 to 2.00) and was predicted by high SES, white race, and longer deceased-donor allograft waiting time in initial DSA.
Conclusions: Ongoing disparities exist in kidney transplantation access and outcomes on the basis of geography and SES despite near-universal insurance coverage under Medicare. Inter-DSA travel improves access and is more common among high SES candidates.
Figures
References
-
- Department of Health and Human Services: The “Final Rule”. Available at: http://www.gaonet.gov/special.pubs/organ/appendd.pdf Accessed August 29, 2009.
-
- Roberts JP, Wolfe RA, Bragg-Gresham JL, Rush SH, Wynn JJ, Distant DA, Ashby VB, Held PJ, Port FK: Effect of changing the priority for HLA matching on the rates and outcomes of kidney transplantation in minority groups. N Engl J Med 350: 545–551, 2004 - PubMed
-
- Mitchell BD, Stern MP, Haffner SM, Hazuda HP, Patterson JK: Risk factors for cardiovascular mortality in Mexican Americans and non-Hispanic whites. San Antonio Heart Study. Am J Epidemiol 131: 423–433, 1990 - PubMed
-
- Ellison MD, Edwards LB, Edwards EB, Barker CF: Geographic differences in access to transplantation in the United States. Transplantation 76: 1389–1394, 2003 - PubMed
-
- Roberts JP, Dykstra DM, Goodrich NP, Rush SH, Merion RM, Port FK: Geographic differences in event rates by model for end-stage liver disease score. Am J Transplant 6: 2470–2475, 2006 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
